Challenges in medical waste management amid COVID-19 pandemic in a megacity Dhaka
Abstract
The COVID-19 pandemic has altered global waste generation dynamics, which is a challenging task for poor countries having inefficient waste management system. On an average, 6,180 tons of medical waste (MW) during this COVID-19 pandemic is generated per month in the Dhaka city. This voluminous amount of MW generated in the Dhaka city is remained poorly managed, and thus, posing a serious threat to public health and environment. To protect any risk of spread of SARS-CoV-2 through MW, a concerted and prompt effort from municipal authorities, hospital administration, and concerned non-government organization (NGOs) is needed to adopt new ways of state-of-the-art, safe and cost-effective MW management system for the Dhaka city. Furthermore, research should be directed to find out to find out other potential sources (e.g., inanimate objects or aquatic bodies) of SARS-CoV-2 infections to track it’s spatial and temporal dynamics, and also to get early warning in case of future outbreaks.
INTRODUCTION
The pandemic COVID-19 is a highly transmissible and pathogenic viral disease caused by a novel coronavirus, the SARS-CoV-2 [1-3]. The ending of this deadly pandemic is unknown, and no reliable therapeutic or preventive medicines are available. Use masks and other personal protection equipment are considered major plausible strategies to protect people from this viral disease [4]. Management of COVID-19 related medical waste (MW) is a new challenge for developing countries where the waste management system is inadequate. The Wuhan city of China experienced a more than the five-fold increase of MW generation immediately after COVID-19 emergence [5]. Different megacities, including Manila, Kuala Lumpur, Hanoi, Bangkok, and some United Kingdom cities, experienced similar increases, producing 154 to 280 tons more MW per day than before the pandemic [6-8]. If not properly managed, the waste generated from health care activities can affect the global environment and the community health of humans, domestic and wild animals [9]. It is estimated that about 5.2 million people including 4 million children die every year due to MW related diseases [10]. Recent World Health Organization (WHO) report states that about 25.0% diseases in developing countries are due to improper waste management, leading to environmental pollution and ultimately to diseases [11]. Improper management of waste associated with COVID-19 disease poses a threat to the spread of this highly contagious disease [12].
Dhaka, the capital city of Bangladesh is the most densely megacity (28,410 people living per square kilometer) in the world. People in Bangladesh (163 million people in 147.5 sq. km) have passed a tough time along with the whole world after COVID-19 hits the country in early March 2020. Dhaka city is the hot spot of COVID-19 infection in Bangladesh. The rate of COVID-19 infection in Dhaka (4,857 per million) is 4-fold higher than the average rate of Bangladesh (1,922 per million) [13]. The COVID-19 associated hazardous MW has created a major havoc in the densely populated Dhaka city. The MW generated from the SARS-CoV-2 infected households and quarantine facilities could represent another potential route for the spread of the SARS-CoV-2 [14]. We are perturbed by the blatant disregard for proper disposal of MW when SARS-CoV-2 infections are increasing along with the number of deaths per day [15]. Peoples in Dhaka city are quite aware of their health, and to protect from COVID-19 disease, more than 50% and 30% people of the Dhaka city wear masks and gloves, respectively. The capital city Dhaka is now the hot spot of COVID-19 disease and more than 50.0% dwellers of this city have started to use protective equipment to protect themselves from the SARS-CoV-2 infection. Thus, MW from households and healthcare facilities are tremendously increasing. In Bangladesh, there are around 654 government hospitals and 5055 private hospitals and clinics with 141,903 beds in total, along with an additional 9061 diagnostic center beds, all of which lead to the generation of huge amounts of MW. The average MW generation rate is 1·63–1·99 kg per bed per day in Dhaka [16]. On an average, 206 tons of MW per day is generated in the Dhaka city alone [16], which is indisputably increasing with the increasing rate of SARS-CoV-2 infections (Figure 1).

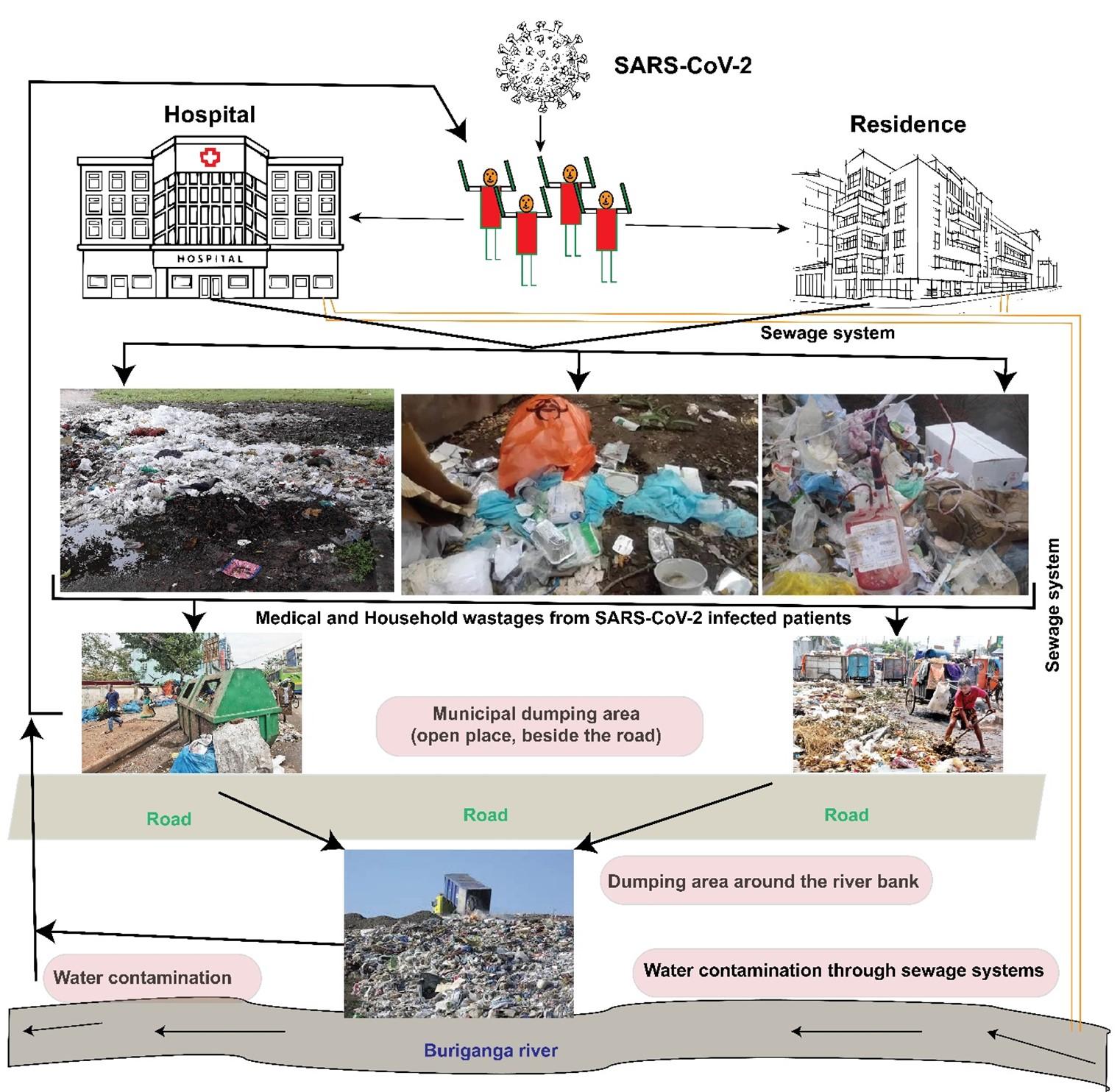
According to Environment and Social Development Organization, 14,165 tons of wastes from single-use plastic was generated in 26 March- 25 April 2020, roughly the first month of COVID-19 infection in Bangladesh [16]. The maximum amount of waste (5,877 tons) was generated from used hand gloves including 3,039 tons from plastic gloves, and 2,838 tons from surgical gloves. In addition, 5,796, 1,592, and 900-tons MW was generated from polythene shopping bags, surgical masks, and used hand sanitizer containers [17]. This voluminous amount of MW generated in the country remained poorly managed, and thus, posing a potential environmental threat, creating a prolonged and unwanted public health hazard, and be a potential source of re-emerging infection (Figure 2).
Most of the hospitals dispose their COVID-19 related MW by mixing them with general waste without sterilization. Moreover, the untrained, unprotected, and unaware cleaners collect the MW, and disposed them in unauthorized places without any separation or proper treatment [16]. Furthermore, owing to lack of the established protected areas for the disposal of MW, the wastes are disposed of in canals or open dumping zone ultimately polluting the environment and contaminate the food chain. In addition to MW, SARS-CoV-2 has been detected in excreta (feces and urine) of infected people, and therefore, wastewater and sewage sludge from infected area can contain SARS-CoV-2 RNA [18, 19]. The SARS-CoV-2 can also survive on plastic and inanimate objects for up to 2-3 days and cause extensive environmental contamination by the confirmed patient [20]. In Dhaka city, all sewage and domestic wastewater are finally discharged to the river Buriganga through various open canals (Figure 2). It poses an additional risk of spread of COVID-19 to Dhaka city.
There are around 5,000 slums in the megacity Dhaka where some of four million slum dwells [21]. During COVID-19 pandemic, more than half of the slum households experiencing illnesses such as fever, cold and other respiratory illnesses [22]. The house-hold waste generated from these slums are not disposed of properly, kept here and there (Figure 2). Therefore, fear of COVID-19 is gearing up among the displaced people in these slums [23, 24].
During the lockdown period, the number of operational waste collectors reduced by almost 50.0% in Dhaka [6]. Though, some non-government organizations (NGOs) namely PRISM Bangladesh Foundation, Nobo Waste Management, Chattogram Seba Songstha and Prodipon etc. have been working as third party by making contracts with the hospitals, but these capacities do not even meet the demands of healthy waste disposal mechanism.
REVIEW RATIONALE AND METHODOLOGY
Till now, thousands of reports on the etiology, origin, genome evolution, molecular diagnosis and vaccine and/or therapeutics of COVID-19 disease have been published. However, literature survey and a comprehensive review on the generation of MW associated with COVID-19, its impact on public health, collection, labelling, disinfection/decontamination and safe disposal are lacking. Therefore, we conducted a rigorous literature survey on the generation, collection, disinfection/decontamination of MW in the megacity of Dhaka, Bangladesh and suggested five key strategic points for its safe disposal. The concept and evidence of public health hazard of MW, and a rationale of this comprehensive review are described in the introduction section. Later sections of this short review were arranged coherently from the literature available in the PubMed central, Google Scholar, ResearchGate, bioRxiv, MedRxiv, Preprints archives, Asian Development Bank (ADB), World Health
Organization (WHO) and online news portals. The literature search was done through screening of titles, abstracts and full articles for eligibility. Proposed strategic points for MW disposal in Dhaka city amid COVID-19 has been represented in Figure 3 which could be used for other megacities of the developing countries of the world.
GLOBAL SCENARIO OF WASTE MANAGEMENT AMID COVID-19
Different countries have adopted different strategies to manage medical wastes generated from healthcare facility and household/quarantine facilities amid this COVID-19 pandemic (Table 1) [25]. Many studies have focused on medical waste management in countries such as Jordan [26], Iran, Egypt, Mauritius [27], Turkey [28], Brazil [29], Mongolia, the United States of America, the United Kingdom, and India [30]. In many developed countries, specific rules and regulations have been implemented for hospital waste management systems and thus, these systems are more effective than those in many developing countries. In many developing countries such as Iran and India, there exists inadequate and insufficient waste treatment facilities as well as protective measures and efficient training of personnel [31].
Norway for instance, allows a temporary change in landfill permit and grants permit to carry waste elsewhere to cope with the medical waste surge. A current debate dealing with this unexpected crisis is to have onsite, mobile or off-site treatment [31]. In China onsite and mobile treatment is considered preferably due to its flexibility in responding to shifting demands. Due to the overwhelming surge in daily waste (i.e., over 240 metric tonnes) and increasing levels of hospital medical waste by sixfold, it is reported that the influx of COVID-19 patients led to the construction of waste plants and deployment of 46 mobile waste treatment facilities in China [32]. In Barcelona, medical waste such as overall, face masks and gloves increased by 350% generating about 1,200 tonnes of medical waste compared to the usual waste of ~ 275 tonnes [33]. Due to the overwhelming tonnes of waste generated during the lockdown, the Irish government announced a million euros funding ring-fenced to tackle the level of illegal dumping attributed to the COVID-19 crisis [34].
Table 1. Medical waste management during COVID-19 in different countries [25].
SUGGESTED MEDICAL WASTE (MW) MANAGEMENT STRATEGIES
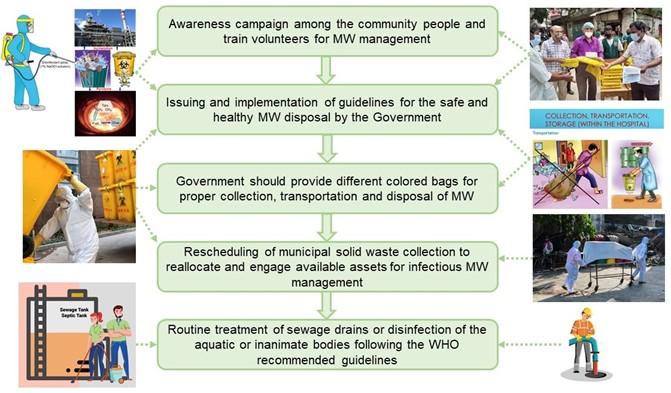
The COVID-19 pandemic has led to an unexpected collapse of waste management chains [35]. Safe and healthy management of MW is crucial to successfully thwarting the disease. Considering the increasing rate of new COVID-19 related MW, we suggest five points strategies as illustrated in Figure 3 for managing the vast amount of MW in Dhaka. First, awareness campaign among the community people including slum dwellers regarding potential hazards of COVID-19-associated MW disposal, and train volunteers, workers, healthcare providers and professionals involved in MW management. Second, urgently issue guidelines for the safe and healthy MW disposal by the government to ensure public health safety. For example, vehicles that carry the MW from healthcare facilities should have a non-absorbent, sealed load area capable of being locked, disinfected, and separate from the driver’s cabin. Third, government should provide yellow medical bags and collection services for proper- (a) wrapping and storing, (b) collection and transportation, and (c) refining and removal of the MW through safe disposal mechanism [6]. Fourth, reschedule municipal solid waste collection frequency according to workforce availability and reallocate available assets for infectious MW management is needed. Fifth, routine treatment of sewage drains or disinfection of the aquatic or inanimate bodies from where the virus can spread should be carried out following the WHO recommended guidelines [36].
These recommendations could be suggested and/or implemented in any other megacity of the developing countries where the MW management systems are very poor, particularly amid COVID-19 pandemic.
CONCLUSIONS AND PERSPECTIVES
In this COVID-19 pandemic situation, safe disposal of MW is now a legal requirement in Bangladesh but lacks in practice. This report discusses current challenges associated MW management strategies in relation to the international guidelines and proposes some strategies to overcome the problems during COVID-19 pandemic. In Dhaka, MW is mainly collected, transported, and managed by municipal agency, hospital authorities, and NGOs. However, the capacities of these stakeholders are not sufficient to comply with the present challenges associated with waste collection, transportation, and environment-safe waste disposal mechanism. A concerted and prompt effort from hospital administration, municipal authorities and other NGO’s is needed to adopt new ways of state-of-the-art, safe and cost-effective MW management system in Dhaka city. Future research should be directed towards the application of the waste-based epidemiology approach, and to find out other potential sources (e.g., inanimate objects or aquatic bodies) of SARS-CoV-2 infections to track the spatial and temporal dynamics of this pandemic, and also to get early warning in case of future outbreaks.
ACKNOWLEDGEMENT
The authors wish to thank the on-line and print media of Bangladesh to bring the concerning issue of medical waste in Bangladesh with data available.
AUTHOR CONTRIBUTIONS
Conceptualization, and drafted the manuscript: GMF and MNH, drafted the manuscript and prepared figures: MSR, and conceptualization, and critically edited the manuscript: MTI.
CONFLICTS OF INTEREST
There is no conflict of interest among the authors.
References
- [1]Hoque MN, Chaudhury A, Akanda MAM, Hossain MA, Islam MT. Genomic diversity and evolution, diagnosis, prevention, and therapeutics of the pandemic COVID-19 disease. PeerJ, 2020, 8, p.e9689.
- [2]Rahman MS, Hoque MN, Islam MR, Akter S, Rubayet-Ul-Alam AS, Siddique MA, Saha O, Rahaman MM, Sultana M, Hossain MA. Epitope-based chimeric peptide vaccine design against S, M and E proteins of SARS-CoV-2 etiologic agent of global pandemic COVID-19: an in silico approach. PeerJ, 2020, 8, pe9572.
- [3]Islam MR, Hoque MN, Rahman MS, Alam ARU, Akther M, Puspo JA, Akter S, Sultana M, Crandall KA, Hossain MA. Genome-wide analysis of SARS-CoV-2 virus strains circulating worldwide implicates heterogeneity. Sci. Rep., 2020, 10(1), 1-9.
- [4]Islam MT, Talukder AK, Siddiqui MN, Islam T. Tackling the Pandemic COVID-19: The Bangladesh Perspective. Preprints, 2020, 2020040384 (doi: 10.20944/preprints202004.0384.v1).
- [5]Si ZH, Li Y. Medical waste treatment in Wuhan from emergency to stability. Xin Hua Net., 2020, pp.2020-04.
- [6]Asian Development Bank (ADB). Managing infectious medical waste during the COVID-19 pandemic, 2020. https://www.adb.org/publications/managing-medical-waste-covid19 (Accessed 23 July, 2020).
- [7]Association of Directors of Environment, Economy, Planning, and Transport, “COVID 19—waste survey results w/c 27 April” 2020.
- [8]Roberts K. P. et al. “Rubbish is piling up and recycling has stalled—waste systems must adapt.” The Conversation, 2020.
- [9]Stuart K, Stewart AG, Wilkinson E, Dobson AE, Edwin MR. A whole systems approach to hospital waste management in rural Uganda. Front. Pub. Health, 2020, 7, p.136.
- [10]The Daily Star. For effective management of medical waste. 05 September, 2020. https://www.thedailystar.net/law-our-rights/law-watch/news/effective-management-medical-waste-1875757 (Accessed 05 September, 2020).
- [11]Trivedi M, Mathur M, Johri P, Singh A, Tiwari, R.K.. Waste management: A paradigm shift. In Environ. Concerns Sustainable Develop., 2020, pp. 337-363, Springer, Singapore.
- [12]Das A, Garg R, Ojha B, Banerjee T. Biomedical Waste Management: The Challenge amidst COVID-19 Pandemic. J. Laboratory Physicians, 2020, 12(2), p.161.
- [13]COVID-19, World Health Organization, Bangladesh. https://www.who.int/docs/default-source/searo/bangladesh/covid-19-who-bangladesh-situation-reports/who-covid-19-update-28-20200907.pdf?sfvrsn=108ef905_2.
- [14]Di Maria F, Beccaloni E, Bonadonna L, Cini C, Confalonieri E, La Rosa G et al.. Minimization of spreading of SARS-CoV-2 via household waste produced by subjects affected by COVID-19 or in quarantine. Sci. Total Environ., 2020, p.140803.
- [15]Uddin MN, Islam MR, Yesmin K. Knowledge on hospital waste management among senior staff nurses working in a selected medical college hospital of Bangladesh. J. Waste Management, 2014, ID 573069.
- [16]ahman MM, Bodrud-Doza M, Griffiths MD, Mamun MA. Biomedical waste amid COVID-19: perspectives from Bangladesh. The Lancet. Global Health, 2020,
- [17]The New Nation. Managing Solid Waste In Covid Time. 17 July, 2020. http://m.thedailynewnation.com/news/258077/complexity (Accessed 23 July, 2020).
- [18]Collivignarelli MC, Collivignarelli C, Miino MC, Abbà A, Pedrazzani R, Bertanza G. SARS-CoV-2 in sewer systems and connected facilities. Process Safety and Environmental Protection, 2020, 143, 196-203.
- [19]Núñez-Delgado A (2020). What do we know about the SARS-CoV-2 coronavirus in the environment?. Sci. Total Environ., 2020, 727, 138647.
- [20]Ong SWX, Tan YK, Chia PY, Lee TH, Ng OT, Wong MSY, Marimuthu K. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. The JAMA., 2020, 323(16),1610-1612.
- [21]Mallick B. Bangladesh slums and Coronavirus concerns. The Third Pole.net. Retrieved from https://www.thethirdpole.net/2020/02/11/bangladesh-concerns-coronavirus, 2020 (Accessed 12 September, 2020).
- [22]The Daily Star. Dhaka Slums: Where COVID is curiously quiet. https://www.thedailystar.net/frontpage/news/dhaka-slums-where-covid-curiously-quiet-1936293, 2020, (Accessed 12 September, 2020).
- [23]Latif MB, Irin A, Ferdaus J. Socio-economic and health status of slum dwellers of the Kalyanpur slum in Dhaka city. Bangladesh J. Sci. Res., 2020, 29(1), 73-83.
- [24]Arias-Granada Y, Haque SS, Joseph G, Yanez-Pagans M. Water and sanitation in Dhaka slums: access, quality, and informality in service provision. The World Bank, 2020.
- [25]ISWA, WASTE MANAGEMENT DURING THE COVID-19 PANDEMIC ISWA’s Recommendations, no. April. 2020.
- [26]Abdulla F., Abu Qdais H., Rabi A. “Site investigation on medical waste management practices in northern Jordan,” Waste Management, 2008, 28(2), 450–458, doi: 10.1016/j.wasman.2007.02.035.
- [27]Mohee R. “Medical wastes characterization in healthcare institutions in Mauritius,” Waste Management, 2005, 25(6), 575–581, doi: 10.1016/j.wasman.2004.10.003.
- [28]Birpinar M. E, Bilgili M. S., Erdoǧan T., “Medical waste management in Turkey: A case study of Istanbul,” Waste Management, 2009, 29(1), 445–448, doi: 10.1016/j.wasman.2008.03.015.
- [29]Da Silva C. E., Hoppe A. E., Ravanello M. M., Mello N. “Medical wastes management in the south of Brazil,” Waste Management, 2005, 25(6), 600–605, doi: 10.1016/j.wasman.2004.03.002.
- [30]Patil AD., Shekdar AV. “Health-care waste management in India,” Journal of Environmental Management, 2001, 63(2), 211–220, doi: 10.1006/jema.2001.0453.
- [31]Ugom M. “Managing Medical Wastes During the COVID-19 Pandemic in Nigeria,” International Journal of Waste Resources, 2020, 1–7, doi: 10.35248/2252-5211.20.10.386.
- [32]Calma J. “The COVID-19 pandemic is generating tons of medical waste – The Verge.” https://www.theverge.com/2020/3/26/21194647/the-covid-19-pandemic-is-generating-tons-of-medical-waste (accessed Dec. 28, 2020).
- [33]ACR+, “Municipal waste management and covid-19.” https://www.acrplus.org/en/municipal-waste-management-covid-19#data_catalonia (accessed Dec. 28, 2020).
- [34]arkodie S.A., Owusu P.A. “Impact of COVID-19 pandemic on waste management,” Environmental Developmental Sustainability, 2020, doi: 10.1007/s10668-020-00956-y.
- [35]You S, Sonne C, Ok YS. COVID-19’s unsustainable waste management. Science, 2020, 368(6498), p.1438.
- [36]World Health Organization (WHO). Water, sanitation, hygiene, and waste management for SARS-CoV-2, the virus that causes COVID-19: interim guidance, 29 July 2020 (No. WHO/COVID-19/IPC_WASH/2020.4) (Accessed 12 September, 2020).
- [37]United News of Bangladesh; https://unb.com.bd/category/Special/amid-covid-19-pandemic-biomedical-waste-turning-more-hazardous/49165.
- [38]https://www.google.com/search?q=google&source=lmns&bih=625&biw=1349&hl=en&sa=X&ved=2ahUKEwiH_qOQwpHuAhUCh-YKHRDhBuIQ_AUoAHoECAEQAA.