Present scenario of COVID-19 in Bangladesh and government preparedness for facing challenges
Abstract
The COVID-19 pandemic caused by SARS-CoV-2 has been showing a speedy growth in the number of infected patients with a remarkable mortality rate, thus it has become a worldwide public health concern. From March 8, 2020, the virus started spreading in Bangladesh. Since then, people got infected so exponentially that the country positions at the list of top infected countries in the world. Therefore, the objective of this comprehensive review was representing the overall scenario of COVID-19 in different sectors of Bangladesh. Because of insufficient scientific publications, we chose materials published by several agencies, media outlets, newspapers, and policy experts to retrieve details information. Up to 4 March 2021, 547,930 confirmed cases and 8,428 deaths were reported in Bangladesh. An alarming fact is that while the global mutation rate of coronavirus is 7.23 % in average, the rate is 12.6 % in Bangladesh. Although the government ruled preventive strategies such as nationwide lockdown, social distancing, contact monitoring, quarantine, and isolation, it was difficult to implement those due to lack of public awareness, inappropriate attitudes and so on. Moreover, the overburdened healthcare system had a weak response at initial stage because of insufficient healthcare facilities. Consequently, this pandemic affected severely almost all the important sectors of the country, specifically the economy, agriculture, education, and health sector. Hence, focusing on healthcare system, maintaining social distance, and other essential precautions can limit the spread of infection and help to alleviate the severity of this pandemic.
INTRODUCTION
The pandemic of coronavirus disease of 2019 (known as COVID-19) is considered as a potential threat to public health that gained global attention after the 2003 Severe Acute Respiratory Syndrome (SARS) [1], followed by 2012 Middle East Respiratory Syndrome (MERS) [2]. The chance of COVID-19 mortality is around 1% and can kill infants, adults, and elderly people with previous medical issues [3]. The clinical presentation varies from asymptomatic illness to severe respiratory failure and shock [4, 5, 6]. Symptoms include cough, fever, and shortness of breath, and associated with headache, dyspnea, sore throat, myalgia, rhinorrhea, vomiting and nausea to different degrees [4, 5, 7]. Besides, patients also show neurological symptoms such as ataxia, convulsion [8] and some neurological signs such as hemorrhagic stroke, dizziness, psychiatric disturbances, acute necrotizing encephalopathy [9, 10].
On December 29, 2019, the virus emerged in the town of Wuhan, the capital of China’s Hubei province [6, 7]. Since then, the infection spread to other regions of Asia, gradually reaching Europe, North America, South America, Africa and Oceania, rendering it a pandemic by March 2020 [4, 11, 12]. The International Committee of Taxonomy of Viruses (ICTV) classified the novel virus as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [13, 14]. On January 30, the World Health Organization (WHO) categorized the 2019-nCoV virus as the sixth Public Health Emergency of International Concern [15] and announced COVID-19 as a global epidemic on March 11, 2020.
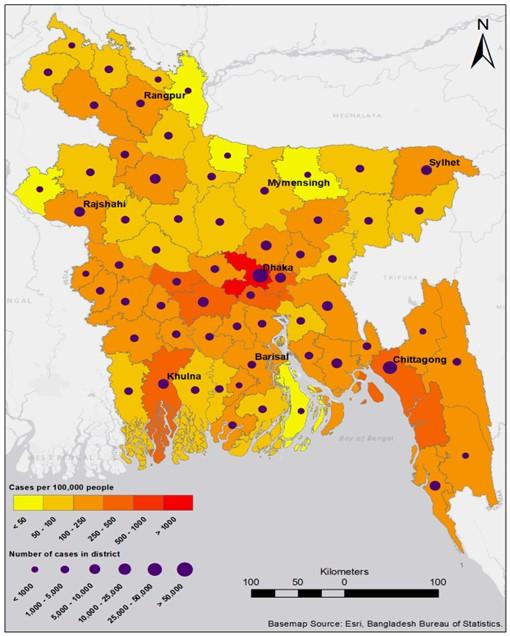
The Institute of Epidemiology, Disease Control and Research (IEDCR), a research institute for monitoring COVID-19 in Bangladesh, first confirmed three reported cases of COVID-19 on March 8, 2020 [16]. Immediately, the government declared a nationwide lockdown on March 22 for 10 days (March 26 to April 04) [17]. Government of Bangladesh (GoB) has agreed to deploy armed forces since 24 March to promote social distance and disease prevention [18]. Until the end of March, infection was low but experienced a steep increase in April [19]. The disease growth percentage in Bangladesh became the highest in Asia on April 11 [20]. On June 13, the number of cases in Bangladesh outpaced the number of cases in China [21], whereas on September 11, the total death number became 4,668 surpassing the total death number of China [22]. Moreover, different districts of the country experienced variable scenario in terms of COVID-19 cases (Figure 1 and Table 1).
In 2020, the economy of Bangladesh has witnessed a drop of 6 percentage points from 2019 due to the lockdown [23]. Resource constraints and inadequate medical facilities, insufficient testing facilities, personal protective equipment (PPE) and other protection measures also created barriers to combat Covid-19. Besides, public awareness and attitude, social distancing challenges, price hike and natural disasters made the crisis more difficult. A study by the Bangladesh Council of Scientific and Industrial Research (BCSIR) revealed that the mutation rate of Coronavirus in Bangladesh was 12.6 %, while the present global average is 7.23 % [24].
CIRCUMSTANCES DURING COVID-19 IN BANGLADESH
In Bangladesh, COVID-19 is a humanitarian concern for public health. The crisis has triggered panic-buying, racism, and mistrust even in places where cases were not officially confirmed, or few cases were reported [25]. However, inconveniences and sufferings that appeared in Bangladesh during this pandemic situation are represented below:
Mass panic among people
Though media portals transmitted substantial updates to mass individuals, it provoked negative consequences. For example, mass panic was highly visible even before announcing the first case from Bangladesh: breaking down of family relationships; patients and staff fleeing from a hospital after an immigrant with flu-like symptoms was admitted [26]. Bangladesh also faced panic buying, terror, social stigma and hate during the lockdown. Mass panic is usually a consequence of misinformation, rumors, exaggeration, and fake news circulated in different social media platforms. Owing to the fear of infection, family doctors, clinics and hospitals in residential and remote areas were also shut down.
Table 1. District wise COVID-19 confirmed cases in Bangladesh up to 15 December 2020 (Institute of Epidemiology, Disease Control and Research. Available from: https://iedcr.gov.bd).
Social distancing challenges
Implementation of the WHO recommended social distancing is difficult in congested regions, especially in marginal communities [27]. In a heavily populated country like Bangladesh, strict social isolation is very difficult to enforce. There are many factors, including close proximity of residents, lack of healthcare concern, inadequate preparation, etc. Maintaining adequate distance is a major challenge for the residents sharing common kitchen, toilets, and corridors [28]. Among the 49.5 million economically active workers, there are a large percentage of daily wage earners for whom the lockout is a curse. Besides, the garments industry, the second largest clothing supplier in 2017 with an earning of USD 29 billion, has been a significant obstacle against social distancing [29].
Public awareness and attitude towards pandemic
Building Resources Across Communities (BRAC) survey (March 31 – April 05, 2020) revealed that around 40% of the respondents are unaware of avoiding infection [30]. Despite the lockdown, many of the people were disobeying the rules. Garment employees walked the streets for getting their unpaid wages [31]. Surprisingly, about 100,000 people attended a funeral of a famous Muslim cleric, rejecting calls from multiple places to retain physical distance and hygiene [32]. In print and online media, many other violations inside and outside the capital city were also reported, including excessive public meeting and roaming without excuse [33]. The risk is exacerbated by thousands of Bangladeshi returning from countries affected by COVID-19 [34].
Rohingya refugees
Bangladesh hosts about 1 million Myanmar Rohingya refugees, with approximately 626,500 residing inthe Kutupalong-Balukhali Expansion Site [35]. With more than 46,000 inhabitants per square kilometer, this location may be considered one of the densest settlements on earth [36]. The 84% refugees reported not having concern about water, sanitation, and hygiene [37]. Every four out of ten children in the camps are afraid to die or lose a friend at COVID-19 [38]. On 9 April, GoB announced a lockdown in Cox’s Bazar and directed prohibitions, but refugees are still arriving in Bangladesh [39]. Despite the preventive measures, first cases were detected in Rohingya camps on 14 May [40].
Effects on economic sector
Due to closing international borders, the scarcity of raw material sources and orders cancellation created a burden on Bangladesh. Readymade Garments Industry (RMG) got the attention because of the cancellation of nearly $3 billion worth of work-orders that may affect approximately 4 million people directly involved in this industry [41]. Banks in Bangladesh were suffering before the pandemic; the situation is becoming vulnerable day by day. Most pharmaceuticals companies also experienced a slump in sales, except for a few top ones. Drugs were not sold much, with the exception of those for hyperacidity, fever and cold [42]. Besides, the prices of basic commodities increased at a noticeable rate because of some unscrupulous traders who raised prices. The airline industry also experienced considerable negative effects due to the cancellation of every international and domestic flight. According to the International Air Transport Association (IATA), revenue loss of this sector may become USD 252,000,000 due to the outbreak [43]. Besides, according to the SANEM forecast, the poverty rate in Bangladesh will increase from 20.5% to 40.9% if Covid-19 leads to a 25% decrease in family income. Consequently, the successes over the past two decades in alleviating poverty can fizzle out [44].
Effects on agricultural sector
Access to agricultural products, materials, markets and advisory services was restricted during the lockdown, which greatly impacted farming. Agricultural processing and trade faced problems with impaired production activities by quarantine measures and low consumer demand, particularly due to limited hotel, restaurant and coffee shop operations [45]. Owing to logistical bottlenecks, farmers are still facing difficulties with having mineral fertilizers, veterinary supplies, and machinery spare parts. The country’s fish and dairy farmers are now bearing their brunt. Crab, shrimp, and fish farmers faced export restrictions, resulting in major economic losses. Exports from Bangladesh constitute more than 70% of crabs in the Chinese market. The export ban in China is a big setback for the crab industry [46]. Additionally, the prices of fruits, cattle and other agricultural products are also dropping. According to the Food and Agriculture Organization (FAO), the pandemic is causing major economic downturns linked to rising of hunger. It is necessary to avoid any distortions in the supply chain during harvest and to ensure food security during the second half of the year while planting spring crops in May and June.
Effects on education sector
Like countries around the world, Bangladesh also closed educational institutions since March to inhibit the spread of COVID-19. However, after extending it for several times, on 22 February 2021, it was announced that public and private universities will start in-person education from 24 May 2021, while the decision regarding reopening of schools and colleges is still to take [47]. After the closing of institutions, extreme uncertainty flourished among students [48], and above 3.15 million tertiary students faced this doubtfulness [49]. In this adverse situation, students started to feel anxiety, depression, and self-harm. A recent online based study on undergraduate level students revealed that 57.5% were mentally stressed, 30.2% had anxiety, and 58.8% were suffering from depression [50]. To tackle this problem, the government declared online education to keep the students in touch with education throughout the pandemic. But, many students could not attend online classes due to lack of resources, internet with low speed, financial inconveniences, and mental instability [51]. Therefore, educationists claimed an irreparable disaster for the education sector because of long-term closure of educational institutions.
Effects on health sector
The public healthcare system in Bangladesh is overburdened. The country spends less than 5 % of it’s Gross domestic product (GDP) on health [52]. China, for example, has a per capita health spending 10 times that of Bangladesh. Health professionals complained of not having sufficient PPE, proper training and other healthcare facilities that created difficulties in coping with the outbreak. Different aspects of healthcare sector of Bangladesh during COVID-19 are briefly represented below:
Quantity and quality of COVID-19 test
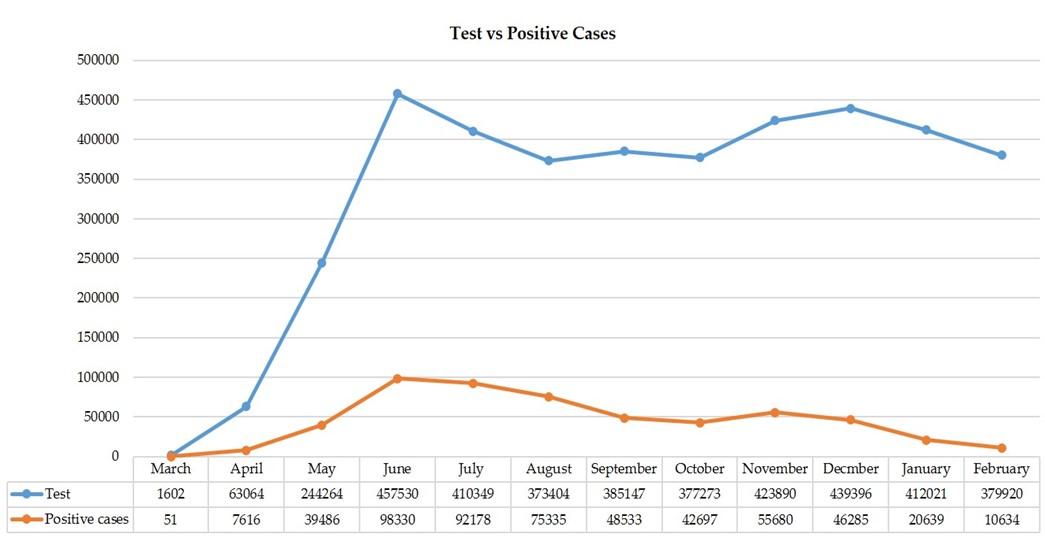
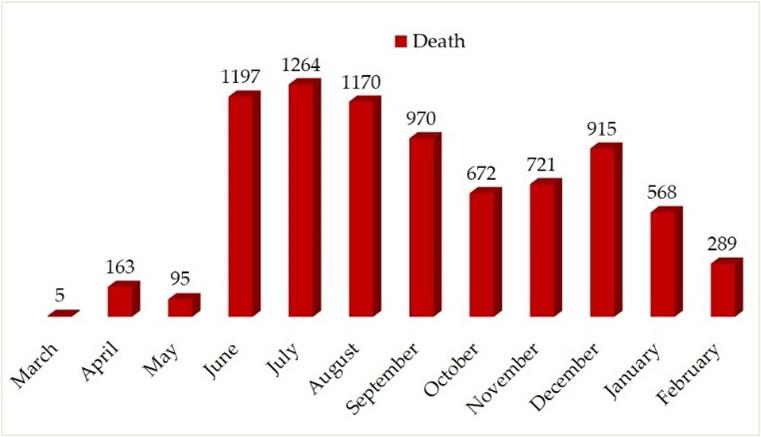
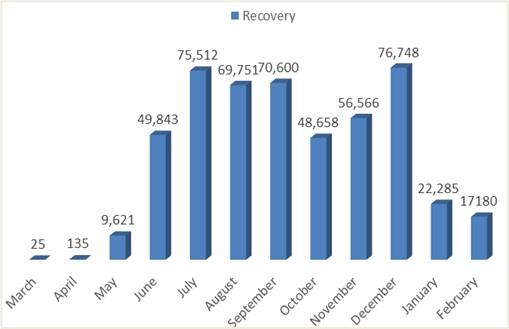
According to IEDCR, on April 18, 2020, the rate of tests per million in Bangladesh was 124, holding the country among the worst performing nations, only above North Korea, Nigeria and Myanmar [53]. Then, with the increase of the number of tests, the number of positive cases increased quickly indicating that many of the patients were not tested and thus caused transmission excessively (Figure 2). As number of positive cases raised, the death rate as well as the recovery rate showed upward trends (Figure 3 & 4). However, all of them, number of tests, positive cases, death rate, and recovery rate, started to fall after December 2020 (Figure 2, 3 & 4). As of 4 March 2021, a total of 4,089,336 tests were performed, reporting 547,930 confirmed cases, of which 499,327 completely recovered and 8,428 died. A total of 94 laboratories throughout the country are performing tests. RT-PCR laboratory test is basically available in these labs. Bangladesh faced a new challenge because, after retesting, false results have been revealed [54]. According to WHO, a retest is required for an accurate result. Dr. Meerjady, director of IEDCR, said, “We do a retest of full samples once a lab begins research. When the laboratory is stable, retesting is steadily decreased” [54]. Meanwhile, a group of Bangladeshi scientists, Dr. Bijon Kumar Sil and his fellow researchers developed a quick low cost ($3.25) test kit that uses the dot blot testing technique to scan for antibodies in the blood [55]. But some scholars including Dr. Kamrul Hasan Khan (a leading Bangladeshi physician) and Dr. Zahidur Rahman (a virologist) doubted the quality, since it had not been certified by international health organizations [55]. However, there are other tests available worldwide that may be employed in Bangladesh to mitigate these drawbacks. For example, genetic sequencing of the blood or respiratory tract swab samples is highly homologous with the known 2019-nCoV, which can be used as diagnosis purpose. Besides, as a key diagnostic instrument, Computed Chest Tomography, [56], as well as serology-based research can be used as parameters of screening [57].
Safety equipment’s and treatment facilities
Unavailability of PPE, masks and hand gloves was the major barrier to effective treatment faced by health service providers. About 4,000 health workers – doctors, nurses, pathologists and technicians – have been infected until June 23 [58]. The mortality rate for physicians was about 4% nationally; the highest in the world, where the overall mortality rate for physicians was 2.5% and experts said low-quality PPE as the primary factor [58]. In Bangladesh, there are a total of 1,169 intensive care unit (ICU) beds, 432 of which are in government hospitals and 737 in private hospitals, compared to 170 million inhabitants [59]. There have 141,903 general hospital beds, means only 0.84 beds for every 1,000 individuals [59]. But the number of ICU beds in the hospitals should be in between 5% and 12% [60, 61]. According to international norms, there should be at least five ICUs in a 100-bed facility [62]. Besides, most of the ICU beds and ventilators are concentrated in the major urban centers, like the Dhaka city making it hard for rural communities to access.
Health service providers
Shortage of Doctors and Nurses is another trouble for Bangladesh. According to the Directorate General of Health Services, there are 93,358 MBBS and 9,569 BDS doctors in the region [63]. According to the new Health Bulletin issued by the Ministry of Health, the country has only six physicians, nurses and midwives for every 10,000 people [64]. Initially, private hospitals were reluctant to treat Covid-19 patients for the safety of other patients and a lack of training of medical personnel [65] though later they started treating. Thus, the patients suffered due to a lack of treatment and the disease spread rapidly. However, the government agreed on April 27 to appoint 2,000 physicians and 6,000 nurses within a week and also 2,654 service providers, including lab attendants, helps, ward boys and conservancy workers for the next six months [66].
Drugs
Several research studies have been running worldwide to develop vaccine or drugs against COVID-19 since the first days. Initially, WHO concentrated on four potential therapies: an experimental compound named remdesivir; the chloroquine and hydroxychloroquine malaria drugs; a combination of lopinavir and ritonavir; and that same combination plus interferon-beta [67]. Next, Russia approved the anti-influenza vaccine, aviifavir [68], the European Medicines Agency (EMA) proposed remdesivir for being approved [69], the UK experts claimed dexamethasone as a major breakthrough [70]. However, a major study including thousands of patients led by the University of Oxford showed hydroxychloroquine is ineffective [71] and studies involving animal models found that favipiravir had a very small effect [72].
While in Bangladesh, physicians have been prescribing multiple medications, including remdesivir and ivermectin [73]. After the UK news of dexamethasone, people in Bangladesh were in a mad rush to purchase the drug, which usually benefited the most severely ill patients requiring respiratory or ventilator support [74]. A Bangladeshi team headed by medical specialist Professor Tarek Alam reported pioneering findings of 100% recovery (60 of 60 patients) within 4 days using ivermectin, antiprotozoal medication and doxycycline as a drug mixture [75]. On 17 June, Bangladesh released these two medications for a clinical trial of 72 infected patients aged between 40 and 65 years with moderate illness for less than 7 days. The results have been good so far, but it still requires detailed research [76].
Convalescent plasma therapy (CPT)
Convalescent Plasma Therapy (CPT) refers to transferring plasma from recovered patients to the infected patients with the same microbes. In this way, antibodies developed in the body of survivors are inserted into the newly diseased bodies, and thus resulting in the passive immunization in the recipients [77]. This technique has been applied in earlier pandemics including Spanish flu, West Nile virus, SARS-CoV, and the Ebola virus7–11. CPT plays a crucial function by lowering the need of ventilator, particularly in low- and middle-class country. Therefore, on 24 March 2020, the FDA approved physicians to use plasma obtained from recovered patients to treat seriously affected COVID- 19 patients [78]. On May 6, at Evercare Hospital Dhaka in Bangladesh, CPT was used to treat a COVID-19 patient for the first time [79]. Then, plasma therapy started to be used at an increased rate in the country. Dhaka Medical College Hospital (DMCH) of Bangladesh led the collection of plasma from survivors and treating of patients using CPT. Dr. MA Khan, head of the Hematology Department, Dhaka Medical College and Hospital (DMCH) encouraged the use of CPT mentioning the therapy as harmless [80]. An online network launched by the GoB and a number of plasma banks also emerged across the country.
Vaccine
To launch the vaccine in Bangladesh, the ambitious efforts of Globe Biotech Ltd. attracted all because the company had successfully conducted a preliminary animal trial [81]. After successful two-phase animal trials in the pre-clinical stage, they were ready to initiate clinical trials of the homegrown vaccine [82]. On the other hand, on November 5, 2020, GoB, Serum Institute of India (SII), and Beximco signed an agreement to import the Oxford-AstraZeneca vaccine. As a result, Beximco Pharma received the first 5 million (another 2 million as a gift from Indian government) AstraZeneca vaccines from the SII on 25 January 2021 [83] and the first vaccination was started on 27 January [84]. After that, the nationwide vaccine inoculation was initiated from 7 February targeting 80% of its population to be inoculated within 6 months [85]. In the first month, the government wanted 6 million people to be vaccinated, but it reduced to 3.5 million doses due to the mistrust, confusion and lack of concern among people [86]. For this reason, spot registration was launched along with online registration and within few days’ registration increased notably. Very few examples of post vaccination side effects were reported. For instance, until 15 February, only 426 people had side-effects among 9,06,033 vaccinated people across the country [87]. However, symptoms such as arm pain and swelling, feverish feeling, tiredness, etc. for few days are not accidental in vaccination because these indicate the response of immunity in building protection.
Alternative medications
COVID-19 has caused a devastating impact worldwide, and there are limited drugs and vaccines available to combat this pandemic. In this adverse situation, several natural therapies can be used as alternatives having no or minimum side effects unlike drugs and vaccines. For example, extract of Nigella Sativa contains different active compounds, including thymoquinone, t‐anetol, ρ‐simen, longifoline, and 4‐terpineol, which showed antiviral, antimicrobial and antitumor activities [88]. A report suggested that N. sativa extract induce Interleukin 8 (IL‐8), and thus it may inhibit SARS‐CoV‐2 virus [89]. Among several ingredients of N. sativa seed, thymiquinone, nigellidine, and α‐hederin might be the efficient herbal drugs against COVID‐19 [90]. Honey can be considered as another alternative because it has protective function to combat various enveloped viruses, and it is also an antagonist for platelet-activating factor (PAF) involving in COVID-19 [91, 92]. By boosting immune response, honey may play a beneficial role in COVID-19 patients [93]. Moreover, there are evidences that vitamin C plays a protective role to fight lung infection [94, 95]. Some recent studies revealed the potential function of vitamin C in COVID-19 patients, suggesting the significance of this type of vitamin [96, 97]. In addition, self- confidence is important for COVID-19 patients which mollify mental stresses caused by the disease, and therefore can strengthen the immune system [98].
Strategy of GoB for COVID-19 confirmed cases
COVID-19 cases have been divided into 4 classes, including mild (Influenza like illness), moderate (pneumonia), severe (severe pneumonia and sepsis), and critical (acute respiratory distress syndrome and septic shock) [99]. Among them, mild and moderate cases are managed at home to undermine the overload of hospitals and evade transmission. These cases can consult doctors by utilizing the telephone or telemedicine services ensured by different government and non-government organizations. On the other hand, severe and critical cases are treated at hospital. Patients with severe symptoms are often provided oxygenation support. Moreover, high dependency unit (HDU) or intensive care unit (ICU) may be required for patients with sepsis. In terms of acute respiratory distress syndrome (ARDS), mechanical ventilation is recommended. Besides, refractory hypoxia patients require ECMO (extracorporeal membrane oxygenation) in ICU setting. During treatment, different therapies are also recommended, such as systemic corticosteroids are prescribed in adults under mechanical ventilation with COVID-19 and ARDS [99]. Several Pharmacological drugs, such as chloroquine, hydroxychloroquine, lopinavir, ritonavir, remdesivir, favipiravir, ribavain and tocilizumab, were indicated for the treatment of patients with pulmonary syndrome without hypoxia [99]. After death of a patient, adequate preventive measures are maintained to prepare and pack the body in a patient room for transferring to an autopsy unit, mortuary, burial site or crematorium. The body is disinfected with 0.05% hypochlorite solution and kept in body bags with resistant of fluid extravasation. People attending to a dead body are provided with proper hand hygiene and personal protective equipment (PPE). The used materials and places are recommended to be cleaned properly to avoid further spreading of COVID-19 [100].
Impact of COVID-19 on children
This pandemic has a significant adverse effect on mental health and development of children, who is going to lead Bangladesh in future. To maintain social distancing, academic institutions have been closed and depended on online based classes. In that lockdown situation, children could interact rarely with their peers and had reduced opportunities of physical activities [101]. As a consequence, they experienced several health problems, including anxiety, sleeping disorder, stress and depression [102, 103, 104]. Moreover, it was predicted that pandemic factors such as increasing infection rate, news of death, lack of environment of gaining knowledge, abnormal behavior of stressed and anxious parents, boredom, and economical damage of family may cause devastating psychological impacts on children [105]. A recent study on children of Bangladesh found that 30.5%, 19.3%, and 7.2% of children had mild, moderate, and severe level of mental disturbances, respectively, during COVID-19 [106]. Therefore, it’s crucial to ensure adequate mental treatment, proper behavior with children, proper nourishment of children, suitable opportunities of physical activities, and financial improvement in order to ameliorate the psychological condition of children of Bangladesh.
LIMITATIONS AND FUTURE DIRECTIONS
Considering the devastating and irreparable damages, Biotechnology may become the blessing for upcoming days to counteract COVID-19 in Bangladesh. Biotechnology has been changing the world through advances in agriculture, medicine, pharmaceuticals, environment and others. While biotechnology is showing it’s blessings in this crisis in medical and pharmaceutical advances, the sector in Bangladesh needs more importance. Every year students of 25 universities in Bangladesh are being involved in several research activities worldwide after doing graduation in Biotechnology. For the first time in Bangladesh, Professor Dr. Samir Kumar Saha, Senjuti Saha and their team from the Child Health Research Foundation (CHRF) sequenced the genome of SARS CoV-2 [107]. Later, many scientists unveiled the genome sequence of the virus, which showed similarity with the viruses of Saudi Arabia, Singapore, Russia, and Australia [107], that opened the milestone to study the virus to produce an effective vaccine against it. More than fifty graduates from the Biotechnology background who hold a graduate or post-graduate degree are serving as frontline fighters on a fully voluntary basis in the country by directly helping to set up laboratories and perform tests [108]. Though they are most eligible ones because of theoretical background and practical experience, they are not considered equally for Covid-19 testing, laboratory setup and any associated technical posts during recruitment. A few days ago, bioengineers from Stanford University developed a technique that suppressed 90% of coronaviruses, called prophylactic antiviral CRISPR in human cells, or PAC-MAN. It consists of an enzyme that destroys the Cas13 virus and a guide RNA strand that tells Cas13 to destroy unique nucleotide sequences in the Coronavirus genome [109]. Genetic Engineers from Bangladesh can come forward with this technique if adequate provisions are provided by the GoB. Besides, computed tomography (CT) of the chest can play a significant role in diagnosis by testing COVID-19 suspects who are negative on qRT-PCR with chest X-ray (CXR) but show medium to high respiratory symptoms [110]. Serology based test, which is detection of antibody specific for SARS CoV2, should also be focused increasingly by following the guidance of CDC as recently antibody test for Covid patients has been approved [111]. Pharmaceutical companies should be supported in the research by GoB for designing drugs or developing vaccine specifically for Bangladeshi variants.
As the deadly COVID-19 is a recent outbreak, some drawbacks have been experienced throughout this study. The lack of availability of adequate data such as scientific publications was one of the noticeable limitations. Therefore, to collect information reflecting the ultimate impacts, numerous materials published by different research agencies, media outlets, policy experts, and newspapers were selected. This review was organized based on themes such as effects of COVID-19 on common people, economic sector, agricultural sector, education sector and healthcare system. However, plenty of more data could be added to each section to represent the COVID-19 situation. Besides, other crucial aspects including transport and communication, politics, tourism, banking, sports, private services, unemployment, poverty, entertainment industry, etc. have not been included in this study.
CONCLUSION
The spread of the SARS CoV-2 has a significant impact on almost all crucial sectors of Bangladesh including economy, agriculture, education and especially the health sector. Inadequate public awareness and attitudes and disobeying social distancing rules have added exceeding obstacles to combat the pandemic. Though the GoB has taken several initiatives such as the lockdown strategy, different stimulus packages, Tk 50 billion granted for the agriculture sector or the noticeable focus on health sector, it has been greatly difficult to fight COVID-19 by this developing country. The government, different organizations, experts like doctors, researchers, biotechnologists as well as the general people must function actively and simultaneously to overcome the devastating effects, while international support is remarkably important (Figure 5). Particularly, emphasizing on the health sector is highly recommended to reduce the demolishing impacts of the pandemic as well as to mitigate the after-effects in Bangladesh.

ACKNOWLEDGEMENT
None.
AUTHOR CONTRIBUTIONS
Conceptualization- MRR, EHS, and AB. Data handling- EHS, IMC, and AB. Original manuscript writing- MRR, EHS, IMC, and AB. Manuscript review and editing- MRR, and RB. GIS mapping- HA. Supervision- MRR, and RB.
CONFLICTS OF INTEREST
There is no conflict of interest among the authors.
References
- [1]World Health Organization (WHO). Summary of Probable SARS Cases with Onset of Illness from 1 November 2002 to 31 July 2003, https://www.who.int/csr/sars/country/table2004_04_21/en/; 2004. [Accessed]
- [2]World Health Organization (WHO). Middle East Respiratory Syndrome Coronavirus (MERSCoV), https://www.who.int/csr/don/2013_12_02/en/; 2013. [Accessed]
- [3]Gates B. Responding to Covid-19—a once-in-a-century pandemic?. N. Engl. J. Med. 2020;382(18):1677-9.
- [4]Chan JF, Yuan S, Kok KH, To KK, Chu H, Yang J, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. The Lancet. 2020;395(10223):514-23.
- [5]Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan , China : a descriptive study. Lancet. 2020;395(10223):507-13.
- [6]Yang X, Yu Y, Xu J, Shu H, Liu H, Wu Y, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. The Lancet Respiratory Medicine. 2020; 395: 497–506.
- [7]hu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020;382: 727–733.
- [8]Baig AM. Neurological manifestations in COVID‐19 caused by SARS‐CoV‐2. CNS NeurosciTher. 2020;26(5):499. doi: 10.1111/cns.13372.
- [9]Li Y, Wang M, Zhou Y, Chang J, Xian Y, Mao L, et al. Acute cerebrovascular disease following COVID-19: a single center, retrospective, observational study.SSRN (Preprint). 2020. doi:10.2139/ssrn.3550025.
- [10]Mao L, Jin H, Wang M, Hu Y, Chen S, He Q, et al. Neurological manifestations of hospitalized patients with covid-19 in Wuhan, China: a retrospective case series study. SSRN 3544840 [Preprint]. 2020.
- [11]CSSE J. Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). 2020-03-15]. https://gisanddata. maps. arcgis. com/apps/opsdashboard/index. html#/bda7594740fd40 299423467b48e9ecf6. 2020.
- [12]Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C, et al. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N. Engl. J. Med. 2020 Mar 5;382(10):970-1. 382, 970–971.
- [13]Gorbalenya AE, Baker SC, Baric R, Groot RJ, Drosten C, Gulyaeva AA, et al. Severe acute respiratory syndrome-related coronavirus: The species and its viruses–a statement of the Coronavirus Study Group. bioRxiv. 2020.
- [14]World Health Organization (WHO). Coronavirus Disease (COVID-2019) Situation Reports, https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports; 2020. [Accessed]
- [15]World Health Organization (WHO). Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV), https://www.who.int/news/item/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov);2020. [Accessed]
- [16]TBS Report. First coronavirus cases detected in Bangladesh. The Business Standard. 2020 March 08.
- [17]Mamun S. “Coronavirus: Bangladesh declares public holiday from March 26 to April 4”. Dhaka Tribune. 2020 March 23.
- [18]Kamruzzaman M. Bangladesh to deploy troops to ensure social distancing. Anadolu Agency. 2020 March 23.
- [19]Nabi MS and Shovon FR. 20-fold rise in Covid-19 cases in Bangladesh since April 1. Dhaka Tribune. 2020 April 14.
- [20]Devulapalli S &Dantewadia P. Mint Covid Tracker: India’s corona trajectory has tapered this week but still remains steeper than Asian peers. Mint. 2020 April 11.
- [21]Tribune Desk. Covid-19: Bangladesh surpasses China with 84,379 confirmed cases, deaths top 1,100. The Dhaka Tribune. 2020 June 13.
- [22]UNB NEWS. Bangladesh’s Coronavirus cases surge to 334,762. UNB. 2020 September 11.
- [23]IMF Country Focus. Helping Bangladesh Recover from COVID-19. IMF News.2020 June 12.
- [24]nline Report. Mutation of coronavirus in Bangladesh faster than global rate: BCSIR study. The Daily Star. 2020 September 06.
- [25]Shimizu K. 2019-nCoV, fake news, and racism. The lancet. 2020 Feb 29;395(10225):685-6. doi: https://doi.org/10.1016/S0140-6736(20)30357-3.
- [26]Kamal RS. “Fear, hatred and stigmatization grip Bangladesh amid Covid- 19 outbreak.” The Business Standard. 2020 March 26.
- [27]Topader RA. COVID-19 threatens to cause a humanitarian crisis. Banglamirrornews. 2020 April 10.
- [28]Ahmed N, Rony RJ, Zaman KT. Social Distancing Challenges for Marginal Communities during COVID-19 Pandemic in Bangladesh. J of Biomed Analytics. 2020 May 21;3(2):5-14.
- [29]BGMEA. “Bangladesh Garments Manufacturers and Exporters Association,”URL http://www.bgmea.com.bd/home/pages/TradeInformation; 2020. [Accessed]
- [30]BRAC. Bangladesh. Rapid Perception Survey On COVID19 Awareness and EconomicImpact, https://reliefweb.int/report/bangladesh/rapid-perception-survey-covid-19-awareness-and-economic-impact-final-draft-may; 2020. [Accessed]
- [31]Reuters. Bangladesh Textile Workers Demand Wages in Protest. The Telegraph. 2020 April 27.
- [32]Mahmud A & Garcia J. 100,000 people gather for funeral in Bangladesh, defying coronavirus lockdown. CNN. 2020 April 19.
- [33]Editorial Desk. Lockdown is a must to contain coronavirus. E-Prothom Alo. 2020 April 08.
- [34]Monjur MR, Hassan MZ. Early phases of COVID-19 management in a low-income country: Bangladesh. Infect Control HospEpidemiol. 2020; 41(9):1116-1117.
- [35]Cousins S. Rohingya threatened by infectious diseases. The Lancet Infect dis. 2018;18(6):609-10.https://doi.org/10.1016/s1473- 3099(18)30304-9.
- [36]UNHCR Mapping Unit. Rohingya Refugee Emergency at a Glance,https://www.arcgis.com/apps/Cascade/index.html?appid=5fdca0f47f1a46498002f39894fcd26f; 2018. [Accessed March 9, 2020].
- [37]Rahman MA, Shamol HH, Griffiths MD, Naher S, Hsan K. Factors associated with the practice of water, sanitation, and hygiene (WASH) among the Rohingya refugees in Bangladesh. J Water SanitHyg Dev. 2019;9(4):794–800.
- [38]Taylor E. COVID-19: forty percent of rohingya refugee children in bangladesh are scared of dying or losing a loved one to the virus. Save the Children. 2020 June 25.
- [39]Kuddus A and Uddin G. Rohingyas at sea for 2months, 32 die. Prothom Alo. 2020 April 17.
- [40]TBS Report. Coronavirus cases detected in Cox’s Bazar Rohingya camps. The Business Standard. 2020 May 14.
- [41]Paul TC. COVID-19 and its impact on Bangladesh economy. The Financial Express. 2020 June 19.
- [42]Noyon AU. A virus that even eats into pharma sector. TBS News. 2020 May 13.
- [43]Deb SK, Nafi SM. Impact of COVID-19 Pandemic on Tourism: Perceptions from Bangladesh. Available at SSRN 3632798. 2020 Jun 22. https://ssrn.com/abstract=3632798 or http://dx.doi.org/10.2139/ssrn.3632798.
- [44]Ahmed HU. Economic ramifications of Covid-19 in Bangladesh. The Financial Express, 2020 May 07.
- [45]Assaubayeva D and Bi Yi PW. Response to Covid-19 for sustainable agriculture transformation. The Financial Express. 2020 May 30.
- [46]Roy R. Covid-19: Increasing economic resilience of the agriculture sector. The Business Standard.2020 May 05.
- [47]Kamruzzaman. Universities in Bangladesh to reopen on May 24. Anadolu Agency. 2021 February 22.
- [48]Zaman NU. Prospects and perils of online education in Bangladesh. New Age. 2020 May 31.
- [49]Ramij M, Sultana A. Preparedness of online classes in developing countries amid COVID-19 Outbreak: A Perspective from Bangladesh. Available at SSRN. https://ssrn.com/abstract=3638718 or http://dx.doi.org/10.2139/ssrn.3638718.
- [50]Banna MH, Sayeed A, Kundu S, Christopher E, Hasan MT, Begum MR, Kormoker T, Dola ST, Hassan MM, Chowdhury S, Khan MS. The impact of the COVID-19 pandemic on the mental health of the adult population in Bangladesh: a nationwide cross-sectional study. International Journal of Environmental Health Research. 2020 Aug 3:1-2. https://doi.org/10.1080/096031 23.2020.1802409.
- [51]Islam MA, Barna SD, Raihan H, Khan MN, Hossain MT. Depression and anxiety among university students during the COVID-19 pandemic in Bangladesh: A web-based cross-sectional survey. PloS one. 2020 Aug 26;15(8):e0238162.
- [52]Khatun F. Health sector cannot be improved only by resources. The Daily Star. 2020 May 11.
- [53]Maswood MH. Bangladesh among lowest testing countries. New Age.2020 Apr 19.
- [54]Mamun S. Covid-19: False positive tests raise concerns. Dhaka Tribune. 2020 April 26.
- [55]Islam A. Are Bangladesh’s low-cost coronavirus test kits reliable? DW News. 2020 April 17.
- [56]Ai T, Yang Z, Hou H, Zhan C, Chen C, Lv W, et al. Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: a report of 1014 cases. Radiol. 2020;296:32-34.
- [57]ang YW, Schmitz JE, Persing DH, Stratton CW. Laboratory diagnosis of COVID-19: current issues and challenges. J of clinical microbiol. 2020;58(6): e00512-20.
- [58]Corraya S. Doctors and health workers die from lack of quality protective equipment. Asia News.2020 June 23.
- [59]Mamun A. Number of ICU beds insufficient to combat Covid-19 pandemic. The Daily DhakaTribune. 2020 March 21.
- [60]Kennedy P, Pronovost P. Shepherding change: how the market, healthcare providers, and public policy can deliver quality care for the 21st century. Crit Care Med. 2006;34(3):1-6.
- [61]Mostafa N. Critical Care Medicine: Bangladesh Perspective. Adv J Emerg Med. 2018;2(3):e27. doi: 10.22114/AJEM.v0i0.79.
- [62]Rungta N, Zirpe KG, Dixit SB, Mehta Y, Chaudhry D, Govil D, Mishra RC, Sharma J, Amin P, Rao BK, Khilnani GC. Indian society of critical care medicine experts committee consensus statement on ICU planning and designing, 2020. Indian J Crit Care Med. 2020;24(Suppl 1):43–60.
- [63]Debnath B &Tajmim T. Doctors, nurses getting sick: Protective gear, curbs on non-essential services can save lives. The Business Standard/ Covid-19 in Bangladesh. 2020 April 16.
- [64]Jahangir AR. Coronavirus: Bangladesh cannot afford losing doctors. UNB News. 2020 April 26.
- [65]Tajmim T. Private hospitals unable, unwilling to treat coronavirus patients. The Business Standard. 2020 March 10.
- [66]Opu MH. Govt to recruit 2,654 health service providers for 6 months. The Dhaka Tribune. 2020May 5.
- [67]Kupferschmidt K& Jon Cohen. WHO launches global megatrial of the four most promising coronavirus treatments. Science. 2020; https://www.utfa.org/content/who-launches-global-megatrial-four-most-promising-coronavirus-treatments. [Accessed]
- [68]Sandberg J. Russians claim to have an effective treatment for the coronavirus, which hospitals will start using this month. Orthospinenews.2020 June 3.
- [69]Euronews. Remdesivir becomes first COVID-19 drug put forward for use in the EU. Euronews.2020 June 25.
- [70]Roberts M. Coronavirus: Dexamethasone proves first life-saving drug. BBC News. 2020 June 16.
- [71]Boseley S. Hydroxychloroquine does not cure Covid-19, say drug trial chiefs.The Guardian. 2020 June 5.
- [72]FavipiravirAnd COVID-19. Favipiravir: Studies Involving Animal Models Shows Favipiravir Has Very Weak Effect On SARS-CoV-2 And Not Viable As An Effective Therapeutic. Thailand Medical News. 2020 Jun 23.
- [73]Masum O. Bangladesh experts advise against using unproven drugs to treat COVID-19. bdnews24.com. 2020 June 01.
- [74]TBS Report. Mad rush for coronavirus drug in Dhaka. The Business Standard. 2020 June 17.
- [75]Singh N. Found effective drug combination to cure Covid-19 patients: Bangladeshi doctors. Hindustan Times. 2020 May 19.
- [76]Press Trust of India. Bangladesh launches clinical trial of two-drug combination to treat Covid-19. Hindustan Times, 2020 June 17.
- [77]Marano G, Vaglio S, Pupella S, Facco G, Catalano L, Liumbruno GM, Grazzini G. Convalescent plasma: new evidence for an old therapeutic tool?. Blood Transfusion. 2016 Mar;14(2):152.
- [78]NPR. FDA Expedites Treatment of Seriously Ill COVID-19 Patients with Experimental Plasma, https://www.npr.org/sections/coronavirus-live updates/2020/03/24/820939536/fda-expedites-treatment-of-seriously-ill-covid-19 patients-with-experimental-pla; 2020. [Accessed]
- [79]Hossain MI. COVID-19: Bangladesh also exploring plasma therapy as a ray of hope. UNB NEWS. 2020 May 23.
- [80]Masum O. Bangladesh experts advise against using unproven drugs to treat COVID-19. bdnews24.com. 2020 June 01.
- [81]FE REPORT. Bangladeshi firm Globe Biotech in race to develop Covid-19 vaccine. The Financial Express. 2020 July 03.
- [82]Hasan J. COVID vaccine: Globe Biotech ready to start clinical trial. The Financial Express.2020 September 12.
- [83]Tribune Report. 5 million Covid-19 vaccine doses arrive in Dhaka. Dhaka Tribune. 2021 January 25.
- [84]News agencies. Bangladesh starts COVID vaccination drive. Al Jazeera. 2021 January 28.
- [85]Reuters.‘The wait is over’: Bangladesh begins COVID-19 vaccinations. Arab News. 2021 February 7.
- [86]Fahmida Khatun. An impressive start to Covid vaccination in Bangladesh. The Daily Star. 2021 February 15.
- [87]TBS Report. 426 cases of Covid vaccine side-effects reported so far. The Business Standard. 2021 February 15.
- [88]Salem ML, Hossain MS. In vivo acute depletion of CD8+ T cells before murine cytomegalovirus infection upregulated innate antiviral activity of natural killer cells. International journal of immunopharmacology. 2000 Sep 1;22(9):707-18.
- [89]Ulasli M, Gurses SA, Bayraktar R, Yumrutas O, Oztuzcu S, Igci M, Igci YZ, Cakmak EA, Arslan A. The effects of Nigella sativa (Ns), Anthemis hyalina (Ah) and Citrus sinensis (Cs) extracts on the replication of coronavirus and the expression of TRP genes family. Molecular biology reports. 2014 Mar;41(3):1703-11.
- [90]Islam MN, Hossain KS, Sarker PP, Ferdous J, Hannan MA, Rahman MM, Chu DT, Uddin MJ. Revisiting pharmacological potentials of Nigella sativa seed: A promising option for COVID‐19 prevention and cure. Phytotherapy Research. 2020 May.
- [91]Semidalas CE, Demopoulos C, Antonopoulou S, Koussissis S. PAF antagonists in food Isolation and identification of PAF antagonists in honey and wax. Etude Rech N4. 1994; 127–32.
- [92]Demopoulos CA. Is Platelet-Activating Factor (PAF) a missing link for elucidating the mechanism of action of the coronavirus SARS-CoV-2 and explaining the side effects-complications of Covid-19 disease?. Preprints. 2020: 2020060253. doi: 10.20944/preprints202006.0253.v1.
- [93]Hossain KS, Hossain MG, Moni A, Rahman MM, Rahman UH, Alam M, Kundu S, Rahman MM, Hannan MA, Uddin MJ. Prospects of honey in fighting against COVID-19: pharmacological insights and therapeutic promises. Heliyon. 2020 Dec 1;6(12):e05798.
- [94]Fowler III AA, Kim C, Lepler L, Malhotra R, Debesa O, Natarajan R, Fisher BJ, Syed A, DeWilde C, Priday A, Kasirajan V. Intravenous vitamin C as adjunctive therapy for enterovirus/rhinovirus induced acute respiratory distress syndrome. World journal of critical care medicine. 2017 Feb 4;6(1):85. doi: 10.5492/wjccm.v6.i1.85.
- [95]Salvayre R, Negre-Salvayre A, Camaré C. Oxidative theory of atherosclerosis and antioxidants. Biochimie. 2016 Jun 1;125:281-296.
- [96]Carr AC. A new clinical trial to test high-dose vitamin C in patients with COVID-19. Critical Care. 2020 Dec;24(1):1-2.
- [97]Farjana M, Moni A, Sohag AAM, Hasan A, Hannan MA, Hossain MG, Uddin MJ. Repositioning Vitamin C as a Promising Option to Alleviate Complications associated with COVID-19. Infect Chemother. 2020 Dec;52(4):461-477.
- [98]Hannan MA, Islam MN, Uddin MJ. Self-confidence as an immune-modifying psychotherapeutic intervention for COVID-19 patients and understanding of its connection to CNS-endocrine-immune axis. J Adv Biotechnol Exp Ther. 2020;3:14-17.
- [99]National Guidelines on Clinical Management of Coronavirus Disease 2019 (Covid-19), Version 4.0. Disease Control Division. Directorate General of Health Services. Ministry of Health & Family Welfare. Government of the People’s Republic of Bangladesh. 2020 March 30.
- [100]Bangladesh Preparedness and Response Plan for COVID-19. Health Services Division. Ministry of Health & Family Welfare. Government of the People’s Republic of Bangladesh. 2020 July.
- [101]Jiao WY, Wang LN, Liu J, Fang SF, Jiao FY, Pettoello-Mantovani M, Somekh E. Behavioral and emotional disorders in children during the COVID-19 epidemic. The journal of Pediatrics. 2020 Jun; 221:264.
- [102]Dunleavy BP. 20% of children on lockdown in China suffer depression, anxiety, study finds. United Press International. 2020 April 24.
- [103]Ramchandani P. Covid-19: We can ward off some of the negative impacts on children. News Scientist. 2020 April 8.
- [104]Rawstrone A. Survey reveals impact of lockdown on children. Nursery World. 2020 May 1.
- [105]Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, Rubin GJ. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. The lancet. 2020 Mar 14;395(10227):912-20.
- [106]Yeasmin S, Banik R, Hossain S, Hossain MN, Mahumud R, Salma N, Hossain MM. Impact of COVID-19 pandemic on the mental health of children in Bangladesh: A cross-sectional study. Children and youth services review. 2020 Oct 1;117: 105277.
- [107]Tribune Desk. Bangladeshi father-daughter duo sequence coronavirus genome. Dhaka Tribune. 2020 May 20.
- [108]Staff Correspondent. Consider us equally for Covid-19 management jobs: biotech graduates. The Daily Star. 2020 June 15.
- [109]ISAAA. CRISPR Technique 90% Effective in Reducing SARS-CoV-2 Coronavirus, http://www.isaaa.org/kc/cropbiotechupdate/article/default.asp?ID=18157; 2020. [Accessed]
- [110]Garg M, Prabhakar N, Bhalla AS, Irodi A, Sehgal I, Debi U, Suri V, Agarwal R, Yaddanapudi LN, Puri GD, Sandhu MS. Computed tomography chest in COVID-19: When & why? Indian J Med Res. 2021 Jan 6. doi: 10.4103/ijmr.IJMR_3669_20.
- [111]Tribune Report. Covid-19: Bangladesh finally approves antibody test. Dhaka Tribune. 2021 January 24.