Epidemiological comparison of the first and second wave of COVID-19 pandemic in Dhaka, Bangladesh: A cross-sectional study among suspected cases
Abstract
Many countries have been seen two wave patterns of reported cases of coronavirus diseases. Still, a limited number of studies compared the epidemiological attributes of the first wave and second wave of coronavirus diseases 2019 (COVID-19) outbreak. This study was carried out to compare the epidemics of two waves in Bangladesh. This observational study data of suspected cases was collected from June 2020 to April 2021 from a local authorized diagnostic center. From June 27, 2020, to July 27, 2020, was considered as the first wave and from March 20, 2021, to April 20, 2021, was considered a second wave. This period was determined because of observing the highest number of positive cases during that period. Out of 21,359 cases, including 2429 (11.37%) individuals in the first wave and 4989 (23.36%) individuals in the second wave had RT-PCR test for disease confirmation. Among them, 315 people in the first wave and 630 in the second wave were positive for SARS-CoV-2 RNA. Male were more vernalized to the positive case, including 204 (64.8%) and 421 (66.8%) during the first and second waves, respectively. People under 41 found 56.2% positive cases during the first wave while it was 65.6% in the second wave. We also found 128 positive cases among international travelers. In conclusion, a large extent of different epidemiological attributes was found in the second wave compared to the first wave of the outbreaks.
INTRODUCTION
COVID-19 is the most devastating epidemic caused by severe acute respiratory syndrome Corona virus-2 (SARS-CoV-2) was first identified in Wuhan, China, in late December [1]. Coronavirus has spread across the world through international travelers [1] Even experts do not still know how the extent and how long it will continue even what will be the future of this diseases [2]. World Health Organization (WHO) considered the 2019-novel coronavirus the sixth public health emergency regarding international concern on January 30. In Bangladesh the first confirmed case was identified on March 08, 2020 [3] currently, it ranks 26 among the affected countries. Bangladesh experienced a surge in COVID-19 infections between mid-June and mid-July last year with 3000-4000 patients per day. Experts termed this period as the first wave.[4] Although Bangladesh is experiencing the worst situation of the pandemic in April 2021 and the health experts said that is the ongoing period of the second wave of COVID-19 that reached its peak in the first week. The infection percentage growth in Bangladesh became the highest in Asia on April 11, 2020. [4], and on June 13 and the total number of identified cases exceed the number of cases in China [5]. WHO defined a pandemic, consider better control if the infection below 5% and thankfully Bangladesh observe this situation from late august after finish first wave to march 2021 [6].
Although, as an early response to the COVID-19 pandemic, the government of Bangladesh announced the prohibition on normal movement to maintain social distancing from March 26 and extended it up to May 30, 2020, in seven different slots [7]. But because of the long-term lockdown, Bangladesh’s economic growth has experienced a drop of 6% from 2019 [8]. Similarly, as a heavily populated country like Bangladesh strict maintenance of lockdown and enforcement social isolation is very difficult where there are about 49.5 million are economically active daily workers [9]and having our garments industry, the second-largest clothing supplier [10].To tackle the COVID-19 situation Bangladesh government also closed the educational institute from May 24, 2021, and after extending several times, the same decision is reached to May 29 2021 [11].But different studies find that this situation adversely affected the student’s mentality they started anxiety, depression, and self-harm [12].Similar containment strategies such as stick lockdown, restricted movement have been taken during the second wave pattern of the COVID-19 pandemic in March – April 2021.
The COVID-19 may vary depending on the underlying comorbidities (diabetes, heart diseases, hypertension, COPD), age, sex, and geographic locations in both waves [13]. Even though Coronavirus can affect individuals, the risk is severe for people aged 60 years or more with comorbidities like cardiovascular sicknesses, constant respiratory infections, diabetes, and malignancy. In Bangladesh, there are approximately 10,742,500 people aged 60 years or above. This huge number of older people indicates a very much vulnerability to COVID -19 as the virus is spreading across the country [3].
The proportion of men contracting the infection was 2.5 which are more than women; men rule the outdoor activities and are less cautious towards staying aware of individual cleanliness. [13] The death rate among males was found higher in various studies around the world, men’s infections rates (71%) and deaths (77%) than females [13]. The infection rate and the death rate also showed a significant difference during the two waves in different territories around the world.
Different countries have been experienced two wave patterns of the COVID-19 reported cases with the first wave in spring and the second wave in late summer and autumn [14]. In Spain, they also experienced two waves pattern of COVID-19 pandemic in which the first wave began from early March 2020 and the second wave was from late August [15]. While South Korea has been depicted the second wave of COVID-19 from August to September 2020 and third wave from November 2020 to January 2021, the new cases were increased. In Iran, during the first wave, they required more respiratory support [16] Compared to their second wave. Although Bangladesh has been experiencing two wave patterns of the COVID-19 pandemic, the epidemiological attributes of the two waves are hardly found. However, the understanding of the characteristics of two waves is necessary not only for this country, but also for the world to get a concept about the COVID-19 wave scenario and taking the early accurate containment strategy to mitigate the virus transmission.
We aim to investigate the epidemiological characteristics of the two waves of the COVID-19 situation in Bangladesh. Here we evaluated the age, gender, rate of COVID-19 positivity, confirmed COVID-19 case in different seasons among the test sample. This study is carried out to give an insight into the epidemiological sorts of the pandemic in Bangladesh. The more important strong point of this study is its uniqueness in exploring the differences of two waves of the COVID-19 outbreak regarding Bangladesh’s perspective.
MATERIALS AND METHODS
Data collection
We conducted a prospective study on suspects who tested RT-PCR for SARS-CoV-2 of a government-recognized local diagnosis center from June 27, 2020, to April 20, 2021. A total of 21358 samples were tested during this period. We collected the data included age, gender, nationality, and their living division in Bangladesh. The suspected whose nasopharyngeal specimens were positive for SARS-CoV-2 RNA using real-time polymerase chain reaction (RT-PCR) has been considered as the positive case. Tests were carried out by isolating mRNA by Auto extraction machine with genolutuon followed by the sentinel Real-Time PCR detection kit (STAT-NATRCOVID-19 B, Italy).
Study design
The start points for both the first and second wave were defined during the time of highest infection and fatality was observed. We took a total of both 30 days during the peak time of infection in Bangladesh for analysis of two waves. We considered the first wave from June 15, 2020, to July 15, 2020, and the second wave from March 15, 2021, to April 15, 2021. Although the second wave was predicted to occur from late March because of taking similar time duration, we calculated the period from March 15, 2021. And after April 15, 2021, the second wave also carried out a couple of days. To analyze the prevalence of COVID-19 among age groups, we categorized the suspect age with 20 years interval. We also determined the possible age groups with their gender preference of infectivity through cross-tabulation analysis.
We also analyzed the test result of those who tested themselves before going abroad or after arrival in Bangladesh to observe the prevalence of infection rates among the international travelers. Here we analyzed a total of about 3263 suspect cases who were international travelers.
And finally, we categorized our suspect’s data according to our season. Bangladesh has a temperate climate condition because of its physical location. It is called the land of six seasons consist of summer (mid- April to mid-June), the rainy season (mid-June to mid-August), autumn (mid-August to mid-October), late autumn (mid-October to mid-December), winter (mid-December to mid-February), and the spring (mid-February to mid-April). We analyzed the data through categorizing with seasonal level to predict the possible infection rate of coronavirus associated with the season.
Statistical analysis
Data were given as an actual number and text format. Statistical data analysis was performed by using PASW statistic software version 18. Some of the analysis was also performed in Microsoft Excel software.
RESULTS
Total population
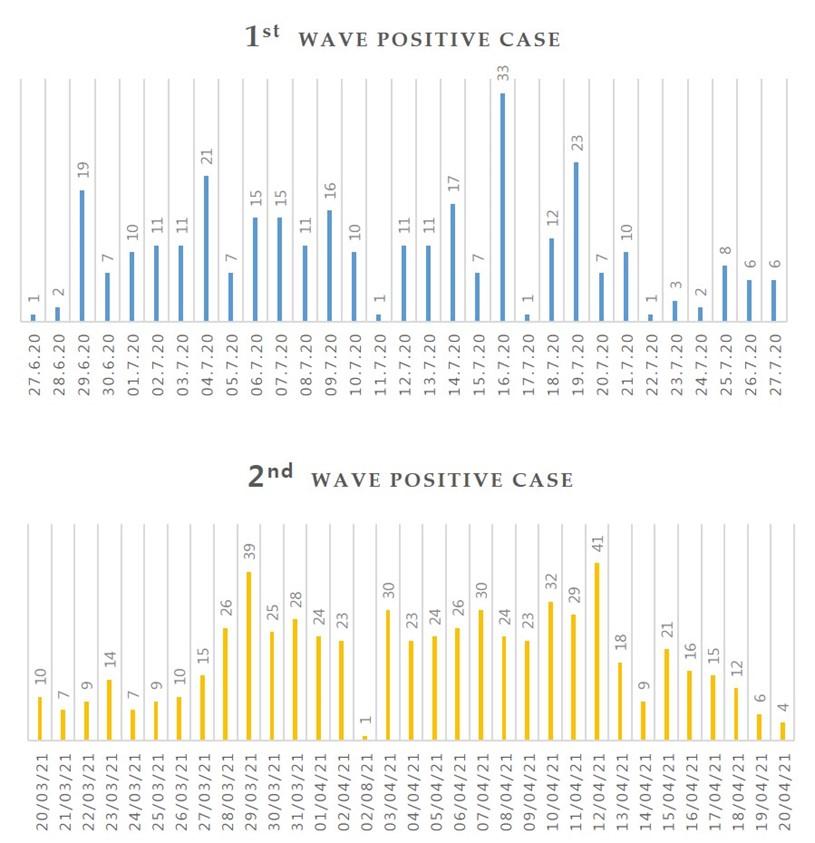
During our data collection period a total of 21,359 suspected cases were tested for COVID-19 from our data collection center. Among them, 17046 (79.8%) were male, and 4313 (20.2%) were female. (Table 1) A total number of 1637 (7.7%) cases were positive for COVID-19 by conforming through the RT-PCR. (Table 2) Day’s wise distribution of positive cases with COVID-19 has been depicted in Figure 1 for both waves.
Table 1. Gender frequency and percentage of total suspects.
Table 2. Test result frequency and percentage of all suspects.
Infected cases during two different waves
2429 (11.37%) cases were tested during the first wave of the COVID-19 epidemic, and 4989 (23.36%) were tested during the second wave. It shows that the rough number of suspects tested during the second wave of the diseases was 2.05% more than the suspect people during the first time. Out of 2429 and 4989 cases, 315 people in the first wave and 630 people in the second wave were examined positive for SARS-CoV-2 RNA, respectively (Table 3).
Table 3. Comparison of epidemiological view between the first wave and second wave of the coronavirus diseases (Covid-19) pandemic in Bangladesh. (Analysis of collected data).
Gender distribution among positive cases
Among 315 confirmed cases with COVID-19 in the first wave, 204(64.8%) individuals were males and 111(35.2%) were female; however, this proportion of for male gender was 421(66.8%) and for female gender was 209(33.2%) in second the wave. (Table 3)
Age distribution among positive cases
Age distribution of confirmed cases has been presented in Figure 2. This shows that the highest prevalence of infected cases was highest between the 21- and 40-years age group during both wave periods. The number of positive cases between 1 and 20 years, 21 and 40 years, 41 and 60 years, and 81 and 100 years were 5.1%, 51.1%, 31.4%, 12.4%, and 0%, respectively in the first wave. In the second wave the positive cases between the age 1 and 20 years, 21 and 40 years, 41 and 60 years, 61 and 80 years, and 81 and 100 years were 6.7%, 58.9%, 26.8%, 7%, and 0.6% respectively.
Surprisingly, about 56.2% of individuals were positive below the age of 40 in the first wave, while during the second wave, this number was increased and reached 65.6%. We also find out the age distribution with gender through cross tab analysis which reveals that almost similar number of positive cases was found in both genders for the individuals below the age of 20 (Table 4).
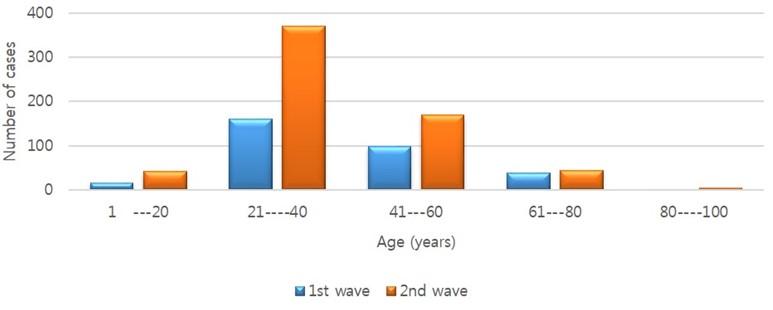
Table 4. Crosstab analysis between age distribution and gender for first wave and second wave.
Positives cases among international travelers
We evaluated the prevalence of positive cases among the international travelers to find out the scenario to spread the coronavirus through them. Here we find a total of 128 positive cases among international travelers. While in the first wave this number was 24(7.6%) which is around 5 times slower than the second wave. Our study also reveals that Indian ranked first with 37 total positive cases among individuals from 80 countries from other national holders. Total 7 positive cases were found in both American and German citizens, 3 positive cases for Chinese and French, 2 for British, Jordanian, Sri Lankan, and a single positive case for Australian, Belgian, Netherlands, Somali, South Korean, Swedish, Turkish and Vietnams (Table 5).
Table 5. Suspect case and the positive case count among international travelers who had test for diseases confirmation.
Seasonal variation among positive cases
Finally, we also find out the season wise variation among the positive cases during our data collection period. The highest positive case was identified in the spring season about 629 cases from 7339 suspects. The percentage of COVID-19 positive was highest in summer season about 12.99% infection case was identified in this season followed by 12.34% in the rainy season, 9.79% in the late-autumn season, 9.37% in spring, 8.23% in autumn and 1.19% in the winter season (Table 6).
Table 6. Seasonal distribution of confirmed cases and the percentage of infection rate.
DISCISSION
A few studies have been performed to compare the epidemiological features of the first and second waves of the COVID-19 pandemic. This study describes the comparative partial scenario of two waves COVID-19 epidemic in Bangladesh. Our result showed that the first wave occurred in June and July, which is relatively moderate warmer months of the year. However, the second wave was beginning in late and was considered a warmer month of the year. Seasonality preference of SARS-CoV-2 is insufficient, but the human coronavirus showed a clear preference for the winter season [17]. COVID-19 data showed temperature region as the prevalence warmer zone [17] and a similar observation is also found in this study so far. Although the wave of optimism by the scientist is that warmer weather might improve COVID-19 situation [18] Respiratory viruses would like to follow seasonal pattern either preferring summer or winter, some of them are year-round virus [17]. In South Korea, they showed that when social activity was increased in the summer, the number of cases grew from middle August. But even maintenance of strengthening of social distancing policies they were experienced with the continued increases case number in November, but this period is the winter season of this country [19].
Different studies reveal that the COVID-19 positive case can be found in any age range even its mortality is about 1% among the infected person and can kill adult, infant and older people with serious medical issues [20]. Whereas in this study, the first wave was venerable for the aged people, but the highest infection cases were observed among young people during the second wave people. Similarly, studies on 100 confirmed cases of COVID-19 patients during the first wave in Iran showed that the average age of the patients was 60.12, where half of them were female. They also found the most common clinical manifestation of the patients were dry cough, fever, dyspnea, anorexia, and fatigue [21]. Although the tendency of infection among males was observed always dominant number during both wave periods. But alternatively, Northern Iran found that women were more vulnerable to this disease during the second wave compared to the first wave to COVID-19 [22].
We also observed the highest numbers of positive cases were identified among Indian travelers who came to Bangladesh during the pandemic period (Table 5). This may occur because a large number of borders have been shared between Bangladesh and India. The risk of infection is also exacerbated by thousands of Bangladeshis returning from other countries affected by COVID-19 [23], especially from India, where a new Variant of coronavirus worsens the situation and WHO listed this variant as a “variant of interest”. Bangladesh has already exposed the infection with Indian variant on April 29 from two men aged 41 and 23 who recently visiting India [24].
Although the characteristics of similarity and difference between the first and second wave of COVID-19 remain unknown in many countries. It is presumed that the incidence of infection of COVID-19 in the early months of the pandemic was much higher than had been reported [25].
Bangladesh has already faced a significant impact on almost all the crucial sectors such as agriculture, education, economy, and particularly in the health sector because of coronavirus spreading with its two waves flow. Although the Bangladesh government has been taking the necessary steps after experiencing the first wave of COVID-19 infection including movement restriction, area wise shut down and so on but the situation was more devastating in the second slot. The possible cause may be the variant of the virus was more infectious compared to the first wave period. A study from the Bangladesh Council of Scientific and Industrial Research (BCSIR) showed that the mutation rate of coronavirus in Bangladesh was 12.6% whereas the current global average is 7.23% [26]. It has been challenging to fight against COVID-19 by this developing country. Apart from this, international support is remarkably important to mitigate this problem, particularly in a developing country like Bangladesh so that the humanitarian crisis does not face during the lockdown period.
The government, different organizations, experts, researchers as well as general public must work actively so that the possible upcoming third wave cannot flow devastatingly in this country. Otherwise, the possible third slot will be more worsen compared to previous times. South Korea is one of the countries which already experienced a long period (more than 56 days) with the third wave compared to 36 days of the second wave. A high level of fatality rate was also exhibited during the third wave compared to the second wave [19]. As the short serial interval (3.9 days) nature and rapid transmissible capability of Coronavirus [27]. Late intervention may have rapid spread in the large community in Bangladesh has to underlie in high risk of the third wave. And studies suggest that late pandemic waves in different periods may be provoked by failure to enforce intervention because of public lassitude [28]. On the other hand, when Bangladesh faced the vaccine crisis and delayed supplying the second dose of the vaccine because of vaccine supplying restriction, the situation would not take a long time to get the worst condition of the pandemic. Although the Bangladesh government is trying their best to mitigate the crisis and importing the vaccine from other countries [26]. As a developing country and having a vast population, Bangladesh needs a long-term strategic plan to tackle the pandemic.
CONCLUSION
In conclusion, the two wave patterns showed quite a different impression regarding infection in Bangladesh, where the second one was more devastating than the first wave. However, prospects are difficult to forecast. But as many countries already experienced with third-wave more badly. At present, the whole world is in the last stage of second wave or perhaps the third wave, as our study indicate the epidemiological features may vary over time it is necessary to know the details information regarding the clinical feature of this disease, mortality rate and other attributes of epidemiological features to co-ordinate the global action to mitigate the crisis. Therefore, if the initial response is taking to delay regarding the third wave of the COVID-19 pandemic, undoubtedly it will be difficult to control the broadcast explosively in local communities.
There have several limitations to this study. Firstly, the full period of the peak time of the second wave does not cover this study while expertise believed that the second wave is still going on. Secondly, other seasonal characteristics like temperature, humidity, and wind were not considered in this study. Thirdly, the genomic variants are one of the main reasons to measure the possible transmission and infection rate that is not included in this study.
ACKNOWLEDGEMENT
The authors are thankful to Dr. Iftekhar Alam for giving some valuable comments during this study.
AUTHOR CONTRIBUTIONS
MMI was involved to design the project. MMI and MFI helped to analyze the data. MSJ helped to collect the data and other information. MFI and MMI both were involved to collect the information. All three authors were involved to write up and final version of the manuscript.
CONFLICTS OF INTEREST
There is no conflict of interest among the authors.
References
- [1]Ali I. COVID-19: Are We Ready for the Second Wave?. Disaster medicine and public health preparedness. 2020, 14(5), e16–e18. doi.org/10.1017/dmp.2020.149
- [2]WHO. Statement on the Second Meeting of the International Health Regulations Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV). January 30 2020.
- [3]https://www.who.int/news/item/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov)
- [4]Islam MM, Rakhi NN, Islam OK, Saha O, Rahaman MM. Challenges to be considered to evaluate the COVID-19 preparedness and outcome in Bangladesh. International Journal of Healthcare Management. 20200(0), 1–2. doi.org/10.1080/20479700.2020.1765120
- [5]Devulapalli S, Dantewadia P. Mint Covid Tracker: India’s corona trajectory has tapered this week but still remains steeper than Asian peers. Mint. 2020 April 11. https://www.livemint.com/news/india/india-s-corona-trajectory-tapered-but-still-remains-steeper-than-asian-peers-11586576536468.html
- [6]Tribune Desk. Covid-19: Bangladesh surpasses China with 84,379 confirmed cases, deaths top 1,100. The Dhaka Tribune. 2020 June 13.
- [7]https://www.dhakatribune.com/bangladesh/2020/06/13/covid-19-deaths-cross-1-100-cases-top-84-000
- [8]Mamun S, Experts: Bangladesh’s second Covid wave has peaked, situation likely to improve in May,DhakaTribune,Monday, May 31, 2021.
- [9]https://www.dhakatribune.com/bangladesh/2021/04/17/experts-bangladesh-s-second-covid-wave-has-peaked-situation-likely-to-improve-in-may
- [10]Shammi M, Bodrud-Doza M, Islam A, Rahman MM. Strategic assessment of COVID-19 pandemic in Bangladesh: comparative lockdown scenario analysis, public perception, and management for sustainability. Environment, development and sustainability. 2020,1–44. Advance online publication.doi.org/10.1007/s10668-020-00867-y
- [11]IMF Country Focus. Helping Bangladesh Recover from COVID-19. IMF News.2020 June 12.
- [12]https://www.imf.org/en/News/Articles/2020/06/11/na-06122020-helping-bangladesh-recover-from-covid-19
- [13]Ahmed N, Rony RJ, Zaman KT. Social Distancing Challenges for Marginal Communities during COVID-19 Pandemic in Bangladesh. J of Biomed Analytics. 2020 May 21;3(2):5-14. doi.org/10.30577/jba.v3i2.45
- [14]BGMEA. “Bangladesh Garments Manufacturers and Exporters Association,” Available at: http://www.bgmea.com.bd/home/pages/TradeInformation; 2020
- [15]ovid: Bangladesh not reopening schools, colleges till May 29,DhakaTribune, May 15, 2021, https://www.dhakatribune.com/bangladesh/education/2021/05/15/bangladesh-not-reopening-educational-institutions-on-may-23-24
- [16]Islam MA, Barna SD, Raihan H, Khan MN, Hossain MT. Depression and anxiety among university students during the COVID-19 pandemic in Bangladesh: A web-based cross-sectional survey. PloS one. 2020 Aug 26; 15(8):e0238162. doi.org/10.1371/journal.pone.0238162
- [17]Siam MHB, Hasan MM, Raheem E, Khan MHR, Siddiqee MH, Hossain MS. Insights into the first wave of the COVID-19 pandemic in Bangladesh: Lessons learned from a high-risk country. MedRxiv. 2020.doi.org/10.1101/2020.08.05.20168674
- [18]Vahidy FS, Drews AL, Masud FN, Schwartz RL, Boom ML, Phillips RA, et al. Characteristics and outcomes of COVID-19 patients during initial peak and resurgence in the Houston metropolitan area. JAMA. 2020; 324: 998–1000. doi: 10.1001/jama.2020.15301.
- [19]Iftimie S, Lo´pez-Azcona AF, Vallverdu´ I, Herna´ndez-Flix S, de Febrer G, Parra S, et al. First and second waves of coronavirus disease-19: A comparative study in hospitalized patients in Reus, Spain. PLoS ONE 2021, 16(3): e0248029. doi.org/10.1371/journal. pone.0248029
- [20]Seyfi S, Amri P, Mouodi S. New modalities for non-invasive positive pressure ventilation: A review article. Caspian J Intern Med. 2019;10(1):1-6. doi:10.22088/cjim.10.1.1
- [21]Moriyama, M., Hugentobler, W.J., Iwasaki, A.: Seasonality of Respiratory Viral Infections. Annual review of virology. 2020. doi:10.1146/annurev-virology- 012420-022445.
- [22]Wang, J., Tang, K., Feng, K., Lin, X., Lv, W., Chen, K.X.et al. : High Temperature and High Humidity Reduce the Transmission of COVID-19. SSRN 2020. doi:10.2139/ssrn.3551767
- [23]Seong H, Hyun Hj, Yun JG, Noh JY, Cheong HJ, Kim WJ and Song JY. Comparison of the second and third waves of the COVID-19 pandemic in South Korea: Importance of early public health intervention. International Journal of Infectious Diseases 2021, 104: 742-745. doi.org/10.1016/j.ijid.2021.02.004
- [24]Gates B. Responding to Covid-19—a once-in-a-century pandemic?. N. Engl. J. Med. 2020;382(18):1677-9. doi: 10.1056/NEJMp2003762
- [25]Javanian M, Bayani M, Shokri M, et al. Clinical and laboratory findings from patients with COVID-19 pneumonia in Babol North of Iran: a retrospective cohort study. Rom J Intern Med. 2020 September 01;58(3):161-167. doi: 10.2478/rjim-2020-0013.
- [26]Jalali SF, Ghassemzadeh M, Mouodi S, Javanian M, Akbari Kani M, Ghadimi R, Bijani A. Epidemiologic comparison of the first and second waves of coronavirus disease in Babol, North of Iran. Caspian J Intern Med. 2020 Fall;11(Suppl 1):544-550. doi: 10.22088/cjim.11.0.544.
- [27]Monjur MR, Hassan MZ. Early phases of COVID-19 management in a low-income country: Bangladesh. Infect Control HospEpidemiol. 2020, 41(9):1116-1117. doi.org/10.1017/ice.2020.147.
- [28]Star Digital Report,Indian variant of Covid-19 found in Bangladesh,The daily star,May 08, 2021,
- [29]https://www.thedailystar.net/coronavirus-deadly-new-threat/news/indian-variant-covid-19-found-bangladesh-2090309
- [30]Yang J, Chen X, Deng X, Chen Z, Gong H, Yan H et al. Disease burden and clinical severity of the first pandemic wave of COVID-19 in Wuhan, China. Nat Commun. 2020, 11: 5411. doi: 10.1038/s41467-020-19238-2.
- [31]Mutation of coronavirus in Bangladesh faster than global rate: BCSIR study. The Daily Star. 2020 September 06.
- [32]https://www.thedailystar.net/coronavirus-deadly-new-threat/news/mutation-coronavirus-bangladesh-faster-global-rate-bcsir-study-1956841.
- [33]Petersen E, Koopmans M, Go U, Hamer DH, Petrosillo N, Castelli F, et al. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect Dis 2020; 20:e238–44. doi.org/10.1016/ S1473-3099(20)30484-9
- [33]Kamruzzaman M,Bangladesh: Uncertainty looms around COVID-19 vaccination,ANADOLU AGENCY,25.04.2021, https://www.aa.com.tr/en/asia-pacific/bangladesh-uncertainty-looms-around-covid-19-vaccination/2219859.