Histological and physiological determinants of hypothyroidism in patients and its relationship with lipid profile
Abstract
Hypothyroidism is a disorder in which the thyroid gland fails to produce enough thyroid hormone to maintain normal physiological function. Low thyroid hormone levels make it difficult for cells in the body to get enough thyroid hormone, resulting in a slowed metabolism. There are various reasons for the prevalence of autoimmune disease and radiation therapy. Excess or deficiency of iodine causes thyroiditis. Because lipids are hydrophobic, they cannot transport fats like cholesterol, phospholipids, and triglycerides through the bloodstream. Instead, they bind to proteins to produce lipoproteins, which carry fats such as cholesterol, triglycerides, and phospholipids throughout the body. This study evaluated the levels of triiodothyronine (T3), thyroxin (T4), and thyroid-stimulating hormone (TSH) in 25 patients and 25 healthy individuals using the EIA technique. The study found that hypothyroidism patients have higher TSH levels than healthy controls, while their T3 and T4 levels are lower than healthy controls. When hypothyroidism patients were compared to healthy controls, there was a significant increase in the mean levels of all lipids except for high-density lipoprotein. We concluded that the TSH levels in hypothyroidism patients were significantly higher than in the control group. In addition, these patients have an abnormal lipid profile, with significantly higher levels of TC, TG, LDL, and VLDL.
INTRODUCTION
Hypothyroidism is a clinical syndrome characterized by a thyroid hormone deficiency, leading to a broad slowdown of metabolic processes [1]. Thyroid dysfunction worsens with advancing age, particularly in women. Numerous biochemical anomalies are linked to hypothyroidism. As thyroid function deteriorates, levels of total cholesterol and low-density lipoprotein cholesterol tend to rise [2].
The thyroid gland generates the hormones triiodothyronine (T3) and tetraiodothyronine (T4), which are essential for human health (T4) and are required for proper energy levels and a healthy lifestyle. Thyroid hormones have long been known to play a role in maintaining the initial concentration of phospholipids in cell membranes and the fatty acid content of lipids [1]. Any effect that lowers the production of T3 and T4 hormones causes hypothyroidism. Hypothyroidism-related abnormal lipid metabolism may lead to atherosclerosis, which may ultimately cause cardiovascular disease. Thyroid disorders are a list of the most frequent endocrine diseases; only diabetes mellitus comes in second [2]. Thyroid disorders are characterized by changes in the number of thyroid hormone production. Hyperthyroidism is caused by excessive production, whereas hypothyroidism is caused by insufficient production [3]. Hypothyroidism is one of the most prevalent thyroid diseases in the world [4]. Thyroid inactivity is caused by decreased T4 and T3 secretion [5]. Low thyroid hormone levels in the blood (hypothyroidism) are related to slowed metabolism, decreased weight gain, lipolysis, poor cholesterol clearance, and high blood cholesterol levels. The effects of thyroid hormone include both genetic and non-genetic [6]. A decrease in T4 and T3 levels causes pituitary TSH hypersecretion and an exacerbated increase in blood TSH levels. In individuals with thyroid dysfunction, changes in lipid profiles are prevalent [7, 8]. The hypothalamic-pituitary-thyroid axis is a system in which the hypothalamus, pituitary, and thyroid work together to govern thyroid hormone synthesis. The hypothalamus gland produces and stores thyrotropin-releasing hormone (TRH). TSH is produced by this hormone, which is then circulated to the thyroid gland, where it increases thyroid hormone synthesis and release [9, 10]. The thyroid gland produces and secretes calcitonin and thyroid hormones. Calcitonin is a hormone that controls calcium levels in the body. Thyroid hormone affects body metabolism, brain development, and other physiological functions. T3 and T4 are often known as thyroxine. Thyroid hormone comes in two metabolically active forms [11]. Hyperthyroidism causes increased metabolism symptoms like hunger, tachycardia, and fatigue.
In contrast, hypothyroidism causes symptoms of a slowed metabolism, including edema, dry skin, and diarrhea. Hypothyroidism is more frequent than hyperthyroidism in thyroid disease, and subclinical thyroid dysfunction is prevalent [12, 13]. There are numerous reasons for hypothyroidism or an underactive thyroid. Some causes include previous thyroid surgery, ionizing radiation exposure, autoimmune thyroiditis, chronic thyroid inflammation, iodine deficiency, a lack of enzymes required to produce thyroid hormone, and numerous medications. Thyroid dysfunction can interfere with thyroid hormone synthesis, a catabolic hormone that affects various metabolic processes, including lipid metabolism. Thyroid hormones regulate cholesterol synthesis, absorption, and metabolism, which helps to maintain a cholesterol reservoir [14]. Thyroid hormones increase the activity of the common effluent treatment plant (CETP), which can influence HDL metabolism. HDL2 cholesteryl esters are switched to very-low-density lipoprotein (VLDL). VLDL and TGs, on the other hand, work in the opposite direction [15, 16]. People with thyroid issues can see the link between thyroid hormones and lipid metabolism. Higher TG and TC levels are associated with overt hypothyroidism. In contrast, overt hyperthyroidism results in lower lipid levels [17]. According to recent molecular biology advancements, thyroid hormones and TSH may play a role in lipid metabolism control. Hypothyroidism is the first stage of severe hypothyroidism, marked by a slight increase in TSH in patients with normal blood T4 levels. In adults, TSH has been linked to hyperlipidemia [18]. Overt hypothyroidism raises total cholesterol (TC) levels in the blood and raises blood pressure (BP). Adults with low FT4 levels have a greater IR, and those with poor thyroid function have a higher risk of CD disease [19]. It’s well known in thyroid conditions, particularly hyperthyroidism and overt hypothyroidism. However, a few studies have found that subclinical hypothyroidism (SCH) causes increased oxidative stress. Thyroid-stimulating hormone (TSH) levels are slightly elevated in SCH, while the rest of the thyroid hormones are normal. As it has the same cardiovascular effects as overt hypothyroidism, it has recently received great attention [20]. Thyroid failure is more common in women and gets more common as you age. TC and LDLC levels are higher in hypothyroid patients [21]. Secondary dyslipidemia is a frequent complication of hypothyroidism [22]. Overt hypothyroidism is associated with increased TC and LDL-C levels [23]. Subclinical hypothyroidism (SH) is more prevalent than overt hypothyroidism. It’s a clinical condition in which blood TSH levels are elevated FT4 yet, and FT3 values are normal. SH is predicted to be present in 4.3 percent to 9% of the general population. Women and the elderly have a greater incidence of SH [24, 25]. Since hypothyroidism and hyperthyroidism are less common in the general population, researchers have increasingly focused on the relationship between thyroid hormones and lipid profiles in the euthyroid population. Free thyroxine (FT4), free triiodothyronine (FT3), TSH, and other hormones are all linked to lipid profiles in the euthyroid population regardless of gender [27]. As a result, the possibility of FT4, FT3, and TSH interacting in their lipid profile link cannot be ruled out. Thyroid hormones were previously thought to mediate TSH’s effects on lipid profile [28]. The current study aimed to find the relationship between lipid profile and thyroid disease as an important factor for diagnosing hypothyroidism, in addition to measuring the histological changing in the thyroid gland as a result of T3 protein expression.
MATERIALS AND METHODS
Sample collection
T3, T4, and TSH levels were evaluated using 5 mL of blood samples collected in a private facility and tested using the enzyme immunoassay technique. A completely automated analyzer was used to assess the blood’s TC, Tg, HDL, LDL, and VLDL cholesterol. Thyroid dysfunction affects lipid metabolism in various ways, including lipid imbalances and carbohydrate and protein abnormalities. Statistical examination of the numerous data collected throughout the study yielded the mean, standard deviation, and P-value for each variable. Between October 2021 and June 2022, Thyroid diseases were evaluated in 25 persons (control samples) who visited a private lab in Babylon province, Iraq.
Ethical statement
Every volunteer has given written informed permission. This research received ethical approval (DSM-6631) for scientific research from the Ministry of Health (MOH) and Ministry of Higher Education and Scientific Research (MOHESR) ethics committees in Iraq.
Samples preparation
Following an overnight fast, blood samples were taken from an arm vein with a disposable syringe and allowed to clot for one hour at room temperature. The serum was separated from the clotted blood in a centrifuge for 5 to 10 minutes at 3000 revolutions per minute (rpm). 10 ml of blood was extracted aseptically from the antecubital vein and transferred to a well-clean and metal-free test tube to prevent hemolysis. The plain test tube was centrifuged for 15 minutes at 2500 rpm after 20 minutes at room temperature. Any leftover erythrocytes were spun down using re-centrifugation, after which the serum was transferred to a polypropylene container and stored until analysis. Half of the serum was transferred to a metal-free test tube, stored at -20°C after proper labeling, and securely packed using well-clean auto pipettes.
A sample of the thyroid gland affected by hypothyroidism was taken and preserved in formalin solution at a concentration of 4% to preserve it from lysis and shrinking. The sample was transferred to jars containing ethanol alcohol (Sigma Aldrich, Germany) with serial concentrations (70%, 80%, 90%, 100%) to prepare the sample. Then it was transferred to other jars containing a solution of xylene (Sigma Aldrich, Germany) at a concentration of 100% to clear the sample and allow the paraffin wax to mix with its sections. After that, the tissue sample was placed in a particular template, and liquid paraffin wax was poured over it at 60°C, then left at room temperature to solidify. Finally, the tissue sections were made at a 5-micron thickness using the microtome device. The sections were loaded on a slide in preparation for the initial dyeing and making of the immunohistochemical assay.
Immunohistochemistry (IHC)
This technique was used to demonstrate hypothyroidism of protein expression. The immunohistochemistry method used for this purpose is the mouse and rabbit specific HRP/DAB detection kit (Abcam, England). This method is summarized by detecting the gene expression product (protein) in the defect T3 and normal cells via targeting the nucleoprotein using human monoclonal antibodies. The binding between primary and secondary antibodies is then detected by immunofluorescent conjugated dye (a polymer-labeled peroxidase). Finally, the positive reaction was determined by the precipitation of blue color at the binding site by the substrate DAB in the chromogen solution [29].
Statistical analysis
All data were analyzed using SPSS software version 16 (SPSS I., Chicago, Illinois, USA) for one-way ANOVA to explore Duncan’s correlation, and means were compared using the L.S.D test. The levels of significance were indicated as p < 0.01 [30].
RESULTS
Effect of thyroid hormones in hypothyroidism
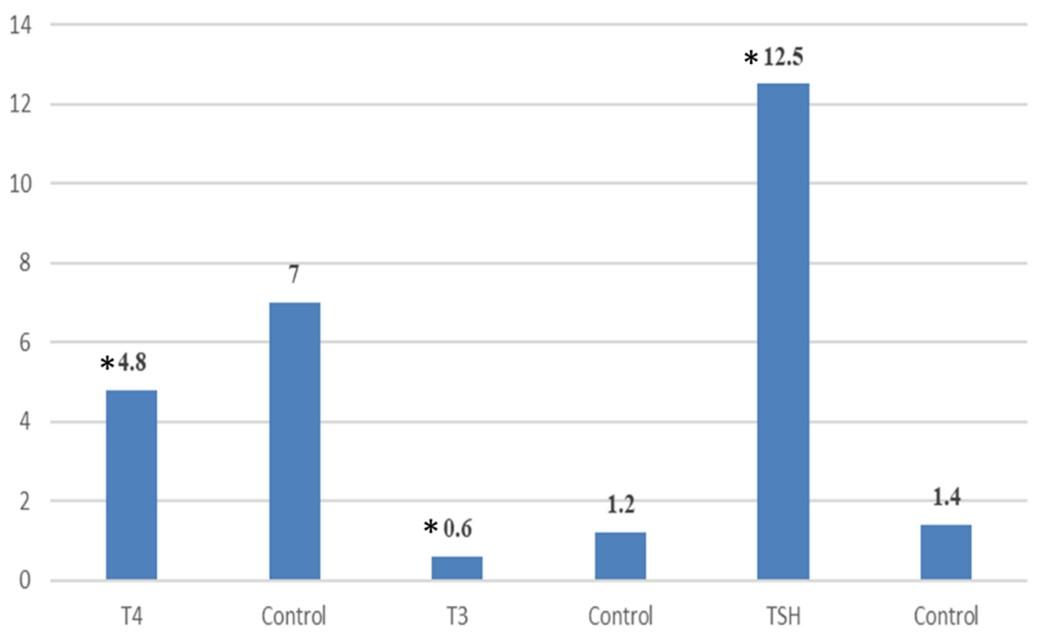
The mean values of T3, T4, and TSH hormones in hypothyroidism and control cases have been studied (Figure 1). TSH levels in hypothyroidism patients were significantly higher in patients (12.5 μIU/L) than in control subjects (1.4 μIU/L). Compared to control, patients experienced a significant drop in T3 and T4 levels.
Effect of lipid profile in hypothyroidism
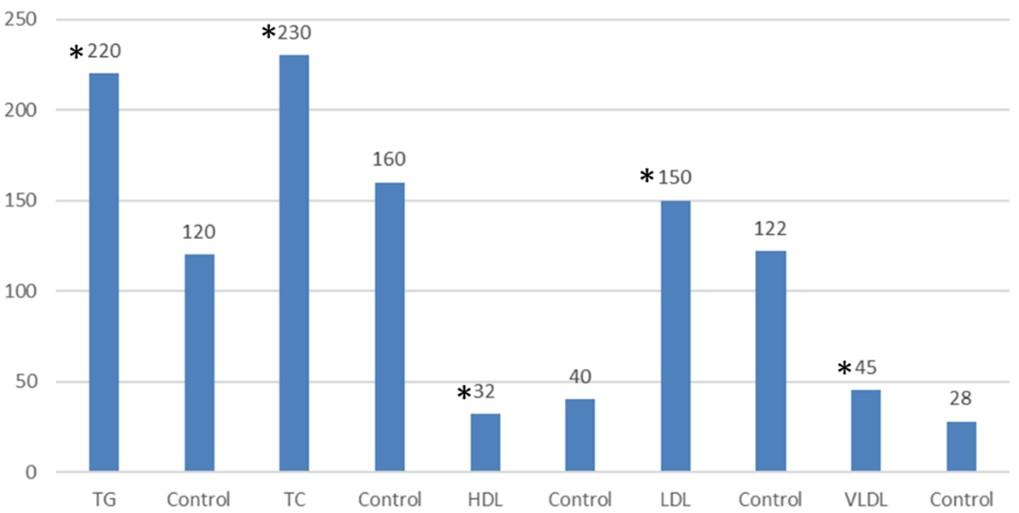
Hypothyroidism patients have an abnormal lipid profile with significantly higher TC, TG, LDL, and VLDL (230, 220, 150, and 45 mg/dI, respectively) (Figure 2). On the other hand, they showed significantly lower HDL activity (32 mg/dI) than control participants (40 mg/dI) (Figure 2).
Expression of T3 in hypothyroidism patients
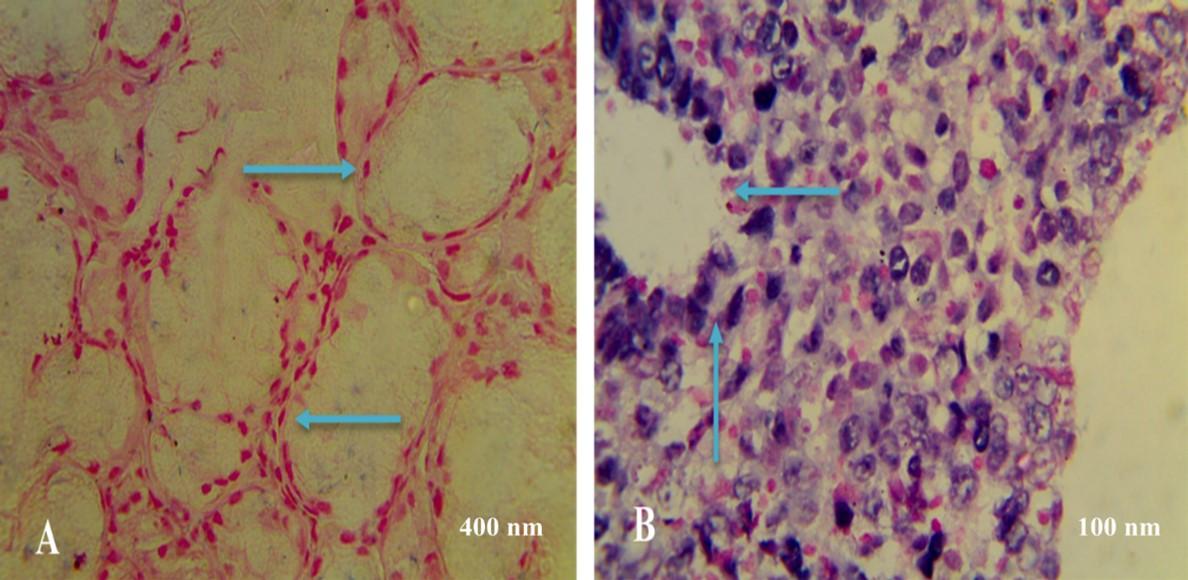
Figure 3 showed the expression of the T3 marker of the thyroid gland during hypothyroidism by IHC. Particularly, Figure 3A showed normal follicle of the gland with stronger IHC reaction and the high signal intensity of normal tissue stained with nuclear fast red stain. While Figure 3B showed swelling of the follicle of the gland as a result of T3 protein expression with moderate IHC reaction and the moderate signal intensity of T3 in hypothyroidism.
DISCUSSION
The thyroid hormone regulates lipid absorption, digestion, synthesis, and catabolism in numerous ways [31]. In overt hyperthyroidism, total cholesterol, LDL-C, and HDL-C (especially HDL2) levels are all reduced, although triglyceride levels are slightly elevated, normal, or decreased [32]. The hypothalamic-pituitary-thyroid system regulates thyroid hormone production. The thyrotropin-releasing hormone is produced and stored by the hypothalamus gland. TSH is produced by this hormone, which is then circulated to the thyroid gland, where it increases thyroid hormone synthesis and release [33, 34]. Thyroid hormone is split into two metabolically active components, T3 and T4, both of which are often referred to as thyroxine [35, 36]. Thyroid function affects the synthesis, mobilization, and breakdown of lipids, among other metabolic factors.
The thyroid hormone increases cholesterol production in the liver. It has a higher conversion rate to bile salts. Thyroid hormone T3 can make adipocytes more sensitive to the lipolytic activity of adrenaline, boosting fatty acid transport to the liver and enhancing hepatic triacylglycerol production indirectly [24, 25]. A lipid profile is a collection of blood tests used to determine the risk of cardiovascular disease. TC, LDL, HDL, VLDL, and triglycerides are all included in this group [21]. VLDL is a kind of lipoprotein that transports fats and cholesterol into circulation. VLDL consists of the most triglycerides compared to the other lipoproteins and is a harmful type of cholesterol [18, 19]. HDL cholesterol was substantially lower in cases compared to controls, whereas total cholesterol, LDL cholesterol, and triglycerides were significantly higher (Figure 2). Lee et al. [19] found that mean plasma total cholesterol and LDL cholesterol levels were higher in hypothyroid patients than in normal controls. The average serum total cholesterol level was higher in both primary and secondary hypothyroidism in another investigation [16, 17]. Laker and Mayes found elevated triglyceride levels in hypothyroid individuals [23]. As a result, the findings of our study were consistent with those of other researchers [34]. The increase in HDL cholesterol concentration is mainly related to increased HDL2 particle concentration [28, 29].
According to Jung and colleagues [31], one of the most common thyroid illnesses in humans is hypothyroidism, a condition in which thyroid hormone production declines due to thyroid gland malfunction, which alters hormone synthesis and secretion. T3 thyroid H&E sections exhibited an increase in the breadth of the follicular epithelium, which was statistically corroborated by a substantial rise in the patients compared to the control group. This was consistent with the findings of another group of researchers, Ferreira et al. [35], who found elevated T3 in the hypothyroid group. In the present study, H&E-stained sections of T3 samples (hypothyroid group) revealed an increase in perifollicular T3 concentration. This might be due to elevated T4 levels caused by increasing TSH levels. These findings were consistent with the findings of Dauth et al. [36], who discovered that hypothyroidism could cause a rise in T4 levels.
CONCLUSION
We concluded that the TSH levels in hypothyroidism patients were significantly higher than in the control group. In addition, these patients have an abnormal lipid profile, with significantly higher levels of TC, TG, LDL, and VLDL.
ACKNOWLEDGEMENT
The authors would like to thank Dr Ameer Mezher Hadi (DNA Research Center, University of Babylon. Pune for their kind support with all laboratory equipment and provide the suitable facilities, also for drafting the manuscript to make this work done.
AUTHOR CONTRIBUTIONS
Conception and design of the study: AMH and YHAM. Drafting the manuscript: SJA and MMB. Analysis and/or interpretation of data: YHAM. All authors read and approved the final version of the manuscript.
CONFLICTS OF INTEREST
There is no conflict of interest among the authors.
References
- [1]Prasad R, Kumar V. Thyroid hormones increase Na+-Pi co-transport activity in intestinal brush border membrane: Role of membrane lipid composition and fluidity. Molecular and Cellular Biochemistry. 2005; 278(1): 195-202.
- [2]Spencer C. Laboratory support for the diagnosis and monitoring of thyroid disease. Pathology. 2009; 41(17).
- [3]Papadopoulos AS, Cleare AJ. Hypothalamic–pituitary–adrenal axis dysfunction in chronic fatigue syndrome. Nature Reviews Endocrinology. 2012; 8(1): 22-32.
- [4]Kumar DV, Mathur DS, Tuteja DR. Effects of thyroid dysfunction on lipid profile. Int J Med Biomed Stud. 2019; 3: 76-80.
- [5]Davis LM, Rho JM, Sullivan PG. UCP‐mediated free fatty acid uncoupling of isolated cortical mitochondria from fasted animals: correlations to dietary modulations. Epilepsia. 2008; 49: 117-119.
- [6]Chin KY, Ima-Nirwana S, Mohamed IN, Aminuddin A, Johari MH et al. The relationships between thyroid hormones and thyroid-stimulating hormone with lipid profile in euthyroid men. International journal of medical sciences. 2014; 11(4): 349.
- [7]Benseñor IM, Goulart AC, Lotufo PA, Menezes PR, Scazufca M. Prevalence of thyroid disorders among older people: results from the São Paulo Ageing & Health Study. Cadernos de saude publica. 2011; 27: 155-161.
- [8]Valeix P, Santos CD, Castetbon K, Bertrais S, Cousty C, et al. Thyroid hormone levels and thyroid dysfunction of French adults participating in the SU. VI. MAX study. In Annales D’endocrinologie. 2004; 65(6): 477-486).
- [9]Dentice M, Salvatore D. Local impact of thyroid hormone inactivation: Deiodinases: the balance of thyroid hormone. Journal of Endocrinology. 2011; 209(3): 273.
- [10]Crook M. Clinical biochemistry and metabolic medicine. CRC Press. 2013. ISBN: 9780429586071.
- [11]Rizos CV, Elisaf MS, Liberopoulos EN. Effects of thyroid dysfunction on lipid profile. The open cardiovascular medicine journal. 2011; 5: 76.
- [12]Lieberman M, Marks AD. Marks’ basic medical biochemistry: a clinical approach (2nd edition). Lippincott Williams & Wilkins. 2009.
- [13]Khan FA, Patil SKB, Thakur AS, Khan MF, Murugan K. Lipid Profile in Thyroid Dysfunction: A Study on Patients of Bastar Tiroid Fonksiyon Bozukluğu .TC, 322(51.19a). 2014; 155-85.
- [14]Peppa M, Betsi G, Dimitriadis G. Lipid abnormalities and cardiometabolic risk in patients with overt and subclinical thyroid disease. Journal of lipids. 2011.
- [15]Roos A, Bakker SJ, Links TP, Gans RO, Wolffenbuttel BH. Thyroid function is associated with components of the metabolic syndrome in euthyroid subjects. The Journal of Clinical Endocrinology & Metabolism. 2007; 92(2): 491-496.
- [16]Cabrera-Solé RM, Lucas CT, Nuñez AG, Luekpe EE, Cañas J, Aguilera M, et al. PO102 subclinical hypothyroidism associates with worst evolution of heart failure in older patients. Global Heart. 2018; 13(4): 407.
- [17]Canaris GJ, Manowitz NR, Mayor G, Ridgway EC. The Colorado thyroid disease prevalence study. Archives of internal medicine. 2000; 160(4): 526-534.
- [18]Luboshitzky R, Aviv A, Herer P, Lavie L. Risk factors for cardiovascular disease in women with subclinical hypothyroidism. Thyroid. 2002; 12(5): 421-425.
- [19]Lee WY, Suh JY, Rhee EJ, Park JS, Sung KC, et al. Plasma CRP, apolipoprotein A-1, apolipoprotein B and Lp (a) levels according to thyroid function status. Archives of medical research. 2004; 35(6): 540-545.
- [20]Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, et al. Serum TSH, T4, and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). The Journal of Clinical Endocrinology & Metabolism. 2002; 87(2): 489-499.
- [21]Wang F, Tan Y, Wang C, Zhang X, Zhao Y, et al. Thyroid-stimulating hormone levels within the reference range are associated with serum lipid profiles independent of thyroid hormones. The Journal of Clinical Endocrinology & Metabolism. 2012; 97(8): 2724-2731.
- [22]Ruhla S, Weickert MO, Arafat AM, Osterhoff M, Isken F, et al. A high normal TSH is associated with the metabolic syndrome. Clinical endocrinology. 2010; 72(5): 696-701.
- [23]Cui CW, Yang SJ, Liu YP, Liu YF. Interaction between p53 and HSP70 in human hepatocellular carcinoma tissues. Chinese Journal of Cellular and Molecular Immunology. 2003; 19(2): 195-196.
- [24]Waheeb AA, Taher MJ, Fahad A, Sarray TR. Thyroid status effect on leptin hormone and lipid profile in female patients with thyroid dysfunction. J. Cardiovasc Disease Res. 2020; 11(4): 200-204.
- [25]Moon HJ, Kwak JY, Kim MJ, Son EJ, Kim EK. Can vascularity at power Doppler US help predict thyroid malignancy? Radiology. 2010; 255(1): 260-269. DOI: 10.1148/radiol.09091284.
- [26]Bishop ML. Clinical Chemistry: Principles, Techniques, and Correlations, Enhanced Edition: Principles, Techniques, and Correlations. Jones & Bartlett Learning 2020.
- [27]Yen PM. Physiological and molecular basis of thyroid hormone action. Physiological reviews. 2001; 81(3): 1097-1142.
- [28]Pagana KD and Pagana TJ. Mosby’s manual of diagnostic and laboratory tests-e-book. Elsevier Health Sciences. 2017. (6th edn).
- [29]Bais R, Michael Bishop, Edward Fody, Larry Schoeff, Baltimore. Clinical Chemistry: Principles, Procedures. Lippincott Williams & Wilkins.2005; 51(8): 1567-1567
- [30]George D, Mallery P. SPSS for Windows step by step: answers to selected exercises. A simple guide and reference. 2003; 63(1): 1461-1470.
- [31]Jung CH, Sung KC, Shin HS, Rhee EJ, Lee WY, et al. Thyroid dysfunction, and their relation to cardiovascular risk factors such as lipid profile, hsCRP, and waist hip ratio in Korea. The Korean journal of internal medicine. 2003; 18(3): 146.
- [32]Laker ME, Mayes PA. Effect of hyperthyroidism and hypothyroidism on lipid and carbohydrate metabolism of the perfused rat liver. Biochemical Journal. 1981; 196(1): 247-255.
- [33]Keyes WG, Heimberg M. Influence of thyroid status on lipid metabolism in the perfused rat liver. The Journal of clinical investigation. 1979; 64(1): 182-190.
- [34]Heimberg M, Olubadewo JO, Wilcox HG. Plasma lipoproteins and regulation of hepatic metabolism of fatty acids in altered thyroid states. Endocrine Reviews. 1985; 6(4): 590-607.
- [35]Ferreira E, Silva AE, Serakides R, Gomes AES, Cassali GD. Model of induction of thyroid dysfunctions in adult female mice. Arquivo Brasileiro de Medicina Veterinária e Zootecnia. 2007; 59: 1245-1249.
- [36]Dauth S, Arampatzidou M, Rehders M, Yu DMT, Führer D, et al. Thyroid cathepsin K: roles in physiology and thyroid disease. Clinical Reviews in Bone and Mineral Metabolism. 2011; 9(2): 94-106.