Prevalence of hyperlipidemia in controlled and uncontrolled type-2 diabetic patients
Abstract
Patients with type-2 diabetes mellitus (T2DM) are known to suffer from hyperlipidemia. How hyperlipidemia is associated with controlled and uncontrolled T2DM patients in Bangladesh remained to be addressed. In this cross-sectional study, 211 participants were enrolled who have been suffering from T2DM for more than 4 years from the northeastern part of Bangladesh. Controlled and uncontrolled patients were defined with their plasma glycated hemoglobin (HbA1c) levels. Among them, 39% and 61% were in the diabetic-controlled and uncontrolled groups. Indeed, the diabetic uncontrolled group showed a higher frequency of hypercholesterolemia, hypertriglyceridemia, hyper LDL-cholesterolemia, and hypo HDL-cholesterolemia compare to the diabetic controlled group. Lipid profiling analysis revealed significantly elevated (p<0.0001) levels of cholesterol, triglyceride, and low-density lipoprotein (LDL) in uncontrolled than the controlled group, while high-density lipoprotein (HDL) was significantly (p<0.0001) lower in uncontrolled diabetics patients. Interestingly, significantly (p<0.05) higher dyslipidemia was also observed in individuals with controlled diabetic population, who have been suffering from T2DM for more than 7 years. Therefore, these results highlight that not only the diabetic uncontrolled but also the controlled group patients have a high risk of developing hyperlipidemia after a certain period of diabetes.
INTRODUCTION
The Lipids, more specifically cholesterol (CHO), triglycerides (TG), phospholipids, lipoproteins are considered essential to the human body by making up the fundamental structure of the cell membrane as a building block and by acting as a precursor to vitamin D, steroid hormones, and bile salts as well as by participating in cell signaling and energy-storing [1-5]. In many unusual physical conditions including diabetes mellitus (DM), the concentration of lipids in human blood has not remained at a normal level which is known as dyslipidemia [6], although the term, hyperlipidemia is a condition that describes only the elevation of lipids such as CHO, TG, lipoproteins, chylomicrons, and LDL within the human body compared to the normal levels [7-9]. Hyperlipidemia is one of the most prevalent non-communicable diseases all over the globe including Bangladesh [10-12].
Hyperlipidemia plays a pivotal role in blood LDL and HDL imbalance which is associated with increased risk of cardiovascular complications [13-17]. Several factors, including diets rich in saturated fats, lower physical activity, obesity, and a few physiological disorders like chronic kidney diseases, biliary obstruction, hypertension, DM, and even pre-diabetic conditions also associated with the increase of hyperlipidemia [18, 19]. Hyperlipidemia is a very common incidence in people with T2DM and prediabetes [20, 21], but the pattern of the different lipid profiles may vary among the ethnic groups, socio-economic levels, and accessibility to the health care system [22, 23].
Various scientific studies have been conducted to establish the prevalence of hyperlipidemia in T2DM patients compared with non-diabetic individuals in various parts of the world. Recent studies in China showed that hyperlipidemia was tremendously common in T2DM patients [24, 25], characterized by increased TG and LDL as well as decreased HDL, and having a high risk of coronary heart diseases [26] when compared to non-diabetic patients. Another Indian research group disclosed that uncontrolled diabetic patients were at high threat of hyperlipidemia and proper glycemic control could prevent it in T2DM patients as well as hinder atherosclerosis and neurological risk [27]. An abnormal lipid profile parameter in T2DM patients is a major risk factor for coronary vascular diseases, which is a combination of T2DM and systemic hypertension [28, 29], revealed by the other two research groups of India and Oman.
However, there were very few studies focused on the prevalence of hyperlipidemia in controlled and uncontrolled diabetic patients. To the best of our knowledge, such type of cross-sectional study has never been conducted in Bangladesh. Therefore, this study aimed to find out the frequency of lipid profile (CHO, TG, HDL, and LDL) in diabetic controlled and uncontrolled groups and analyze the comparative prevalence of hyperlipidemia between the two groups.
MATERIALS AND METHODS
Study population
A total of 211 clinically diagnosed diabetic samples were used to complete this study. The specimens were collected from both male and female patients of more than twenty years old as well as suffered from T2DM for a prolonged period (more than 4 years). Primarily, diabetic patients were categorized into the controlled and uncontrolled groups based on the last 3 years of glycated hemoglobin (HbA1c) history, and that information was collected from the patient’s health record books. HbA1c levels of >6.5% were considered as uncontrolled diabetes group while <6.5% as controlled group [30, 31].
Study place, time, and approval
The study was carried out in the Department of Biochemistry and Molecular Biology of Shahjalal University of Science and Technology, Sylhet-3114, Bangladesh, from July 2019 to August 2021. Few technical supports were taken from a well-known diagnostic center named Medinova Medical Services Ltd. Sylhet, Bangladesh. This study was approved by the Departmental Ethical Committee of the Department of Biochemistry and Molecular Biology of Shahjalal University of Science and Technology, Sylhet-3114, Bangladesh (reference no.: 01/BMB/2019). All the participants of diabetic patients were given a consent form for their approval and after getting their informed consent; a standard questionnaire set was circulated among the study participants to answer. Sociodemographic data were collected by trained medical staff following standardized protocol [32-34] on a structured questionnaire, which contained the responder’s name, ID, address, age, sex, body weight and height, duration of diabetes, type of diabetes, family history, occupation, physical activities, current health status, etc. (attached questionnaire as supplemental file).
Specimen collection and preparation
The specimen was collected from several hospitals and diagnostic centers named MAG Osmani Medical College and Hospital, Diabetic Hospital Sylhet, and Medinova Medical Services Ltd. of a north-eastern city named Sylhet in Bangladesh. The relevant specimen like 3ml of venous blood was collected after overnight fasting from each participant under strict aseptic precautions in different two vacutainer blood collection tubes for desired blood parameters estimation. Both the purple-top tube and red-top tube (serum separator tube) [35-37] was used to collect the whole blood. The whole blood from the purple-top tube was used to estimate the HbA1c level of blood to define the controlled and uncontrolled diabetic patient. Another red-top tube blood was used to separate serum by centrifuging at 4000 rpm and 37℃ for 20 minutes and was used to estimate the levels of CHO, TG, LDL, and HDL.
Biochemical assays
HbA1c estimation: Controlled and uncontrolled diabetic patients were identified through estimating their HbA1c levels from whole blood with an automatic chemistry analyzer (Dimension RxL Max Integrated Chemistry System, SIEMENS, USA) using dimension flex hemoglobin A1c reagent kit (Siemens Healthcare Diagnostics Inc., USA).
Lipid profile estimation: Lipid profile i.e., total CHO, TG, LDL, and HDL were estimated by colorimetric methods using commercially available kits such as Cholesterol liquicolor, Triglycerides liquicolormoto, LDL cholesterol liquicolor, and LDL cholesterol liquicolor (Human Diagnostic, Germany) respectively [32]. All lipid profile measurements were done according to the manufacturer’s protocols (Human Diagnostic, Germany) with a semi-auto biochemistry analyzer (Humalyzer 3000, USA). The accuracy of all the analyses was confirmed through standard calibration regularly.
Statistical analysis
For the statistical analysis, all the data obtained by biochemical assays were added in Microsoft Office Excel 2007. The average and standard deviation were calculated. To define the controlled and uncontrolled diabetic patients, the association of lipid profile in both the controlled and uncontrolled groups and in diabetes duration-based populations, the mean of the variables and student t-test (two-tailed) were used. A p-value of <0.05 was considered statistically significant, otherwise not significant (NS).
RESULTS
Diabetes and HbA1c
In this study, a total of 211 participants were included with their consent, who had been suffering from type-2 diabetes for more than four years. Among the participants, 56% and 44% were male and female, respectively (Table 1). Based on the standard level of HbA1c, the controlled (<6.5%) and uncontrolled (≥6.5%) diabetic patient groups were defined which were 39% and 61% respectively (Table 1). Interestingly, the level of HbA1c was significantly (p<0.0001) higher in uncontrolled diabetic patients than that of the controlled group [Figure 1(A)]. We categorized all the diabetic patients into several age groups wherein 51-60 years old individuals showed more susceptibility to diabetes mellitus [Figure 1(B)].
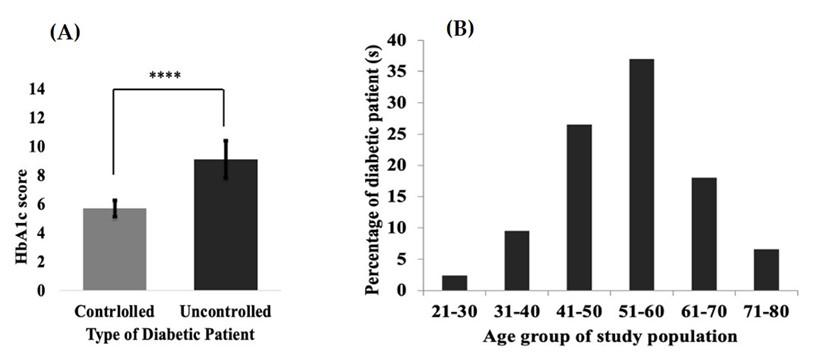
Table 1. Control, uncontrolled, and sex-based sample distribution.
Hyperlipidemia associated diabetes
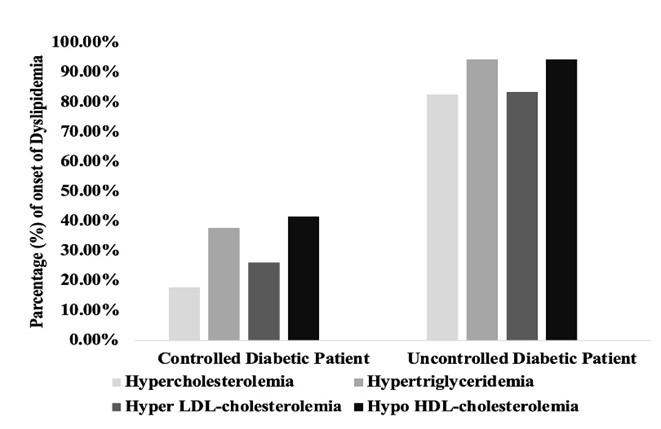
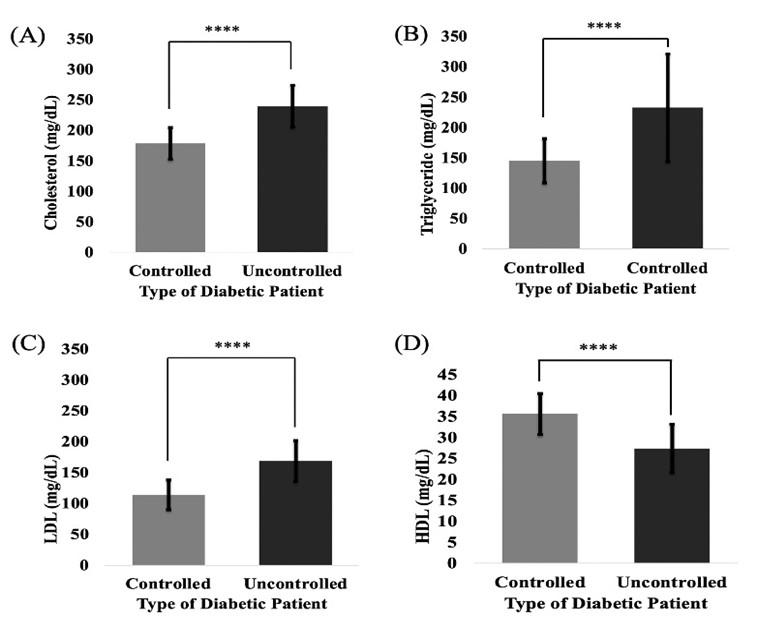
High TG and low HDL levels were observed in patients with type -2 diabetes. The frequency of hypercholesterolemia, hypertriglyceridemia, hyper LDL-cholesterolemia, and hypo HDL-cholesterolemia were 17.80%, 37.70%, 26.20%, and 41.70% respectively, in the diabetes-controlled group (Figure 2). In contrary, the frequencies of the mentioned earlier parameters were quite high in the uncontrolled group representing 82.60%, 94.50%, 83.50%, and 94.50% respectively (Figure 2). T2DM patients generally tend to develop hyperlipidemia and vice-versa. In our study, we have seen a significant (p <0.0001) elevation of serum CHO, TG, and LDL in the diabetic uncontrolled patient group in comparison with the controlled group. Moreover, the uncontrolled group showed significantly (p <0.0001) lower HDL than the controlled group. These results suggest that uncontrolled diabetic patients are at high risk of hyperlipidemia than controlled ones (Figure 3).
Duration-based exploration of lipid profile
We also studied the status of lipid profiles in controlled diabetic patients depending on the onset of the duration of their diabetes. Significantly, (p <0.05) higher CHO and TG were noticed after 7 years of diabetes onset [Figure 4(A), 4(B)] but remarkably elevated LDL was detected after 8 years of diabetes mellitus [Figure 4(C)]. In the case of HDL, significantly lower (p <0.05) levels were observed in the controlled group after 7 years of diabetes mellitus [Figure 4(D]).
DISCUSSION
The present study was conducted to assess the frequency of dyslipidemia in diabetic controlled and uncontrolled groups so that both types of patients would be more aware to lead a healthier lifestyle as well as to control their DM. To the best of our knowledge, this is the first study that reports the prevalence of hyperlipidemia in controlled and uncontrolled diabetic patients in the Bangladeshi population.
This study found that about 61% of the diabetic patients had bad glycemic control which was considered as a diabetic uncontrolled group and the remaining 39% were having good glycemic control and were considered as a diabetic controlled group [30]. An age group of 51-60 years was detected as more susceptible to T2DM. One of the studies conducted in India found 64.5% of diabetic uncontrolled patients from the total population of that study based on standard levels of HbA1c and the majority (41.8%) of diabetic patients of the study population were belonging to the 51-60 age group category [38]. Another two research groups from USA and India reported that T2DM usually appears in middle-aged people (40-60 years) and our results are in line with them [38, 39].
This cross-sectional study revealed an alarming scenario of the high number of patients with hypercholesterolemia (82.60%), hypertriglyceridemia (94.50%), hyper LDL-cholesterolemia (83.50%), and hypo HDL-cholesterolemia (94.50%) based on the standard serum levels of CHO (150-200 mg/dl), TG (50-150 mg/dl), LDL (<130 mg/dl), and HDL (>35 mg/dl) [40, 41] in type-2 diabetic uncontrolled group which were almost 4.5, 2.5, 3, and 2 times higher compared with the controlled group. As in the current studies, high prevalence of cholesterol (up to 72%), triglyceride (up to 70%), and LDL (48%), and lower HDL (up to 37%) have been reported for the South Asian population [42-45] where CHO, TG, and LDL levels in the diabetic uncontrolled group were almost 1.1, 1.3, and 1.7 times higher respectively which are slightly lower than this study.
This cross-sectional study observed significantly (p<0.0001) elevated CHO, TG, and LDL levels in the diabetic uncontrolled group than in the controlled group. Besides, a significantly (p<0.0001) lower level of HDL was also detected in the uncontrolled group compared to the diabetic controlled one. A few of scientific studies from USA, UK, China, and India have reported that they observed higher CHO, TG, and LDL, as well as lower HDL levels in type-2 diabetic patients [42, 46-49], compared to the non-diabetic individuals and the results of this study are in line with them. According to a Sudanese study, overproduction of LDL leads to increase plasma TG and decrease HDL levels in T2DM patients [50] which is analogous to our findings. The pattern of lipid profiles in the uncontrolled and controlled groups of this study is similar to other studies performed in Iraq [51, 52].
Any disorder in carbohydrate metabolism leads to a disorder in lipid metabolism, so high concentration of plasma CHO, TG and decline in plasma HDL levels lead to insulin resistance with or without DM which is intently related to a qualitative change in the lipid profile pattern [53], i.e., plasma lipid profile and hyperglycemia are interrelated which also harmonious to our lipid profiling observations.
The status of lipid profile in controlled diabetic subjects based on the duration of onset of their T2DM was also explored. The controlled group was significantly (p<0.05) susceptible to hypercholesterolemia, hypertriglyceridemia, and hypo HDL-cholesterolemia after 7 years of DM onset. On the other hand, hyper LDL-cholesterolemia was significantly (p<0.05) observed in the controlled group after 8 years of DM. A significant positive correlation between lipid profile (CHO, TG, LDL, and HDL) and duration of diabetes was shown in an Indian scientific study [42], and in this study, we also found significantly (p<0.05) high lipid profile in diabetic controlled group after 7 years of diabetes onset. Recently, a Chinese scientific study revealed that a longer duration of DM was associated with a high risk of cardiovascular diseases by emerging plasma lipid profile [54], although according to another Nigerian study [55], lipid profile pattern did not skew to the duration of diabetes. Throughout the study, we did not consider the food habits of T2DM patients, which is maybe a limitation of this study to analyze the lipid profiles of both the controlled and uncontrolled groups perfectly.
CONCLUSIONS
A significantly higher prevalence of hyperlipidemia was observed in the uncontrolled diabetic population as well as in the controlled group after 7 to 8 years of diabetes onset which is an alarming risk of cardiovascular diseases and other lipid-related complications. Overall, hyperlipidemia is closely associated with a lack of proper management of T2DM and also with the long duration of diabetes. So, not only glycemic control but also the duration of DM should be considered by clinicians to assess hyperlipidemia-related complications. Further research should be carried out using several provable parameters including food habits that may involve with hyperlipidemia in controlled and uncontrolled type-2 diabetic patients.
ACKNOWLEDGEMENT
We acknowledge and thank the SUST research center for funding (grant number LS/2019/01/01) and also thanks to the Department of Biochemistry and Molecular Biology, Shahjalal University of Science and Technology, Sylhet-3114, and to Medinova Medical Services Ltd. Sylhet, Bangladesh for technical support. We are also grateful to MAG Osmani Medical College and Hospital and Diabetic Hospital Sylhet, Bangladesh, for allowing us to collect samples. Finally, we express our deepest sense of gratitude to all participants for their endeavor in this study.
AUTHOR CONTRIBUTIONS
MAH was involved in the conception and design of the experiments. MAH, FRN, AIA, MH, SSP, and PCD contributed to perform the experiments. MAH and MWM analyzed data. MAH contributed to drafting the article. MAH and ZH contributed to revising it critically for important intellectual content. MAH and ZH made the final approval of the version to be published. All authors have read and agreed to the published version of the manuscript.
CONFLICTS OF INTEREST
There is no conflict of interest among the authors.
References
- [1]Andrei CS, Bruno C, Francisco AHF, Marcelo CB, Abrahão AN, et al. IV Diretriz Brasileira sobre Dislipidemias e Prevenção da Aterosclerose. Departa-mento de Aterosclerose da Sociedade Brasileira de Cardiologia. Arq Bras Cardiol. 2007; 88 Suppl I:2-19. doi.org/10.1590/S0066-782X2007000700002.
- [2]Fahy E, Subramaniam S, Murphy RC, Nishijima M, Raetz CR, Shimizu T et al. Update of the LIPID MAPS comprehensive classification system for lipids. J Lipid Res. 2009 Apr;50 Suppl (Suppl): S9-14. doi: 10.1194/jlr. R800095-JLR200.
- [3]Subramaniam S, Fahy E, Gupta S, Sud M, Byrnes RW, Cotter D, et al. Bioinformatics and systems biology of the lipidome. Chem Rev. 2011 Oct 12;111(10):6452-90. doi: 10.1021/cr200295k.
- [4]Dashti M, Kulik W, Hoek F, Veerman EC, Peppelenbosch MP, Rezaee F. A phospholipidomic analysis of all defined human plasma lipoproteins. Sci Rep. 2011; 1:139. doi: 10.1038/srep00139.
- [5]Dashty M, Motazacker MM, Levels J, de Vries M, Mahmoudi M, Peppelenbosch MP, et al. Proteome of human plasma very low-density lipoprotein and low-density lipoprotein exhibits a link with coagulation and lipid metabolism. Thromb Haemost. 2014 Mar 3;111(3):518-30. doi: 10.1160/TH13-02-0178.
- [6]Dixon, Dave L; Riche, Daniel M. “Dyslipidemia”. Pharmacotherapy:A Pathophysiological Approach, 11e. Book authored by Joseph T. DiPiro, Gary C. Yee, L. Michael Posey, Stuart T. Haines, Thomas D. Nolin, Vicki Ellingrod. April 21, 2021.
- [7]Shasha Y, Hongmei Y, Xiaofan G, Xingang Z, Liqiang Z, Yingxian S, et al. Prevalence of dyslipidemia and associated factors among the hypertensive population from rural Northeast China. BMC Public Health (2015) 15:1152. doi:10.1186/s12889-015-2486-7.
- [8]Shattat G. F. A Review Article on Hyperlipidemia: Types, Treatments and New Drug Targets. Biomed Pharmacol J 2014;7(2).
- [9]Hill MF, Bordoni B. Hyperlipidemia. In: StatPearls. StatPearls Publishing, Treasure Island (FL); 2020.
- [10]GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017 Sep 16;390(10100):1151-1210. doi: 10.1016/S0140-6736(17)32152-9.
- [11]Murray CJ, Ezzati M, Flaxman AD, Lim S, Lozano R, Michaud C, et al. GBD 2010: a multi-investigator collaboration for global comparative descriptive epidemiology. Lancet. 2012 Dec 15;380(9859):2055-8. doi: 10.1016/S0140-6736(12)62134-5.
- [12]Karthikeyan G, Teo KK, Islam S, McQueen MJ, Pais P, Wang X, et al. Lipid profile, plasma apolipoproteins, and risk of a first myocardial infarction among Asians: an analysis from the INTERHEART Study. J Am Coll Cardiol. 2009 Jan 20;53(3):244-53. doi: 10.1016/j.jacc.2008.09.041.
- [13]Cooney MT, Dudina A, De Bacquer D, Wilhelmsen L, Sans S, Menotti A, et al. HDL cholesterol protects against cardiovascular disease in both genders, at all ages and at all levels of risk. Atherosclerosis. 2009 Oct;206(2):611-6. doi: 10.1016/j.atherosclerosis.2009.02.041.
- [14]Nelson RH. Hyperlipidemia as a risk factor for cardiovascular disease. Prim Care. 2013 Mar;40(1):195-211. doi: 10.1016/j.pop.2012.11.003.
- [15]Ahmed HM, Miller M, Nasir K, McEvoy JW, Herrington D, Blumenthal RS, et al. Primary Low Level of High-Density Lipoprotein Cholesterol and Risks of Coronary Heart Disease, Cardiovascular Disease, and Death: Results From the Multi-Ethnic Study of Atherosclerosis. Am J Epidemiol. 2016 May 15;183(10):875-83. doi: 10.1093/aje/kwv305.
- [16]Briel M, Ferreira GI, You JJ, Karanicolas PJ, Akl EA, Wu P, et al. Association between change in high density lipoprotein cholesterol and cardiovascular disease morbidity and mortality: systematic review and meta-regression analysis. BMJ. 2009 Feb 16;338: b92. doi: 10.1136/bmj. b92.
- [17]Stamler J, Daviglus ML, Garside DB, Dyer AR, Greenland P, Neaton JD. Relationship of baseline serum cholesterol levels in 3 large cohorts of younger men to long-term coronary, cardiovascular, and all-cause mortality and to longevity. JAMA. 2000 Jul 19;284(3):311-8. doi: 10.1001/jama.284.3.311.
- [18]Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2016 Jan 26;133(4): e38-360. doi: 10.1161/CIR.0000000000000350.
- [19]Huang Y, Cai X, Mai W, Li M, Hu Y. Association between prediabetes and risk of cardiovascular disease and all-cause mortality: systematic review and meta-analysis. BMJ. 2016 Nov 23;355: i5953. doi: 10.1136/bmj. i5953.
- [20]Mooradian AD. Dyslipidemia in type 2 diabetes mellitus. Nat Clin Pract Endocrinol Metab. 2009 Mar;5(3):150-9. doi: 10.1038/ncpendmet1066.
- [21]Santos-Gallego CG, Rosenson RS. Role of HDL in those with diabetes. Curr Cardiol Rep. 2014 Sep;16(9):512.
- [22]Gerber PA, Spirk D, Brändle M, Thoenes M, Lehmann R, Keller U. Regional differences of glycaemic control in patients with type 2 diabetes mellitus in Switzerland: a national cross-sectional survey. Swiss Med Wkly. 2011 Jul 7;141: w13218. doi: 10.4414/smw.2011.13218. PMID: 21735364.
- [23]Joshi SR, Anjana RM, Deepa M, Pradeepa R, Bhansali A, Dhandania VK. Prevalence of dyslipidemia in urban and rural India: The ICMR-INDIAB study. PLoS ONE. 2014, 9, e96808. https://doi.org/10.1371/journal.pone.0096808.
- [24]Yan L, Xu MT, Yuan L, Chen B, Xu ZR, et al. Prevalence of dyslipidemia and its control in type 2 diabetes: A multicenter study in endocrinology clinics of China. J Clin Lipidol. 2016; 10:150–60.
- [25]Devrajani B R, Shah SZA, Soomro AA, Devrajani T. Type 2 diabetes mellitus: A risk factor for Helicobacter pylori infection: A hospital-based case-control study. International journal of diabetes in developing countries. 2010, 30(1), 22.
- [26]Yang Z, Xing X, Xiao J, Lu J, Weng J, et al. Prevalence of cardiovascular disease and risk factors in the Chinese population with impaired glucose regulation: the 2007–2008 China national diabetes and metabolic disorders study. Experimental and clinical endocrinology & diabetes: official journal. German Society of Endocrinology and German Diabetes Association. 2013; 121:372–4.
- [27]Smita G, Rajat M, Ankit G. Lipid profile pattern in controlled and uncontrolled diabetic patientsin a tertiary care centre. Int J Res Med Sci. 2020 April; 8(4):1528-1531.
- [28]Sreenivas RA, Meera S, William E, Kumar JS. Correlation between glycemic control and lipid profile in type 2 diabetic patients: HbA1c as an indirect indicator of dyslipidemia. Asian J Pharm Clin Res 2014;7(2):153–155.
- [29]Al-Alawi SA. Serum lipid profile and glycated hemoglobin status in Omani patients with type 2 diabetes mellitus attending a primary care polyclinic. Biomed Res 2014;25(2):161–166.
- [30]Catherine CC, Keith FR, Danita DB, Edward WG, Earl SF, Linda SG, et al. Prevalence of Diabetes and High Risk for Diabetes Using A1C criteria in the U.S. Population in 1988–2006. Diabetes Care Mar 2010, 33 (3) 562-568; doi:10.2337/dc09-1524.
- [31]International Expert Committee. International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care. 2009;32(7):1327–1334. doi:10.2337/dc09-9033
- [32]Ali N, Rahman S, Islam S, et al. The relationship between serum uric acid and lipid profile in Bangladeshi adults. BMC Cardiovasc Disord 19, 42 (2019). doi.org/10.1186/s12872-019-1026-2.
- [33]Haque T, Rahman S, Islam S. et al. Assessment of the relationship between serum uric acid and glucose levels in healthy, prediabetic and diabetic individuals. Diabetol Metab Syndr 11, 49 (2019). doi.org/10.1186/s13098-019-0446-6.
- [34]Saadi MM, Roy MN, Haque R. et al. Association of microalbuminuria with metabolic syndrome: a cross-sectional study in Bangladesh. BMC Endocr Disord 20, 153 (2020). doi.org/10.1186/s12902-020-00634-0
- [35]Van Dongen-Lases EC, Cornes MP, Grankvist K, Ibarz M, Kristensen GB, Lippi G, et al. Patient identification and tube labelling – a call for harmonisation. Clin Chem Lab Med. 2016 Jul 1;54(7):1141-5. doi: 10.1515/cclm-2015-1089.
- [36]Bayot ML, Tadi P. Laboratory Tube Collection. [Updated 2021 Aug 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555991/
- [37]Simundic AM, Cornes MP, Grankvist K, Lippi G, Nybo M, Ceriotti F, et al. Colour coding for blood collection tube closures – a call for harmonisation. Clin Chem Lab Med. 2015 Feb;53(3):371-6. doi: 10.1515/cclm-2014-0927. PMID: 25324449.
- [38]Shanmuga P, Nasreen B. Correlation of Lipid Profile with Duration of Diabetes and HbA1c Levels in Type 2 Diabetes Mellitus Patients: A Descriptive Cross-sectional Study. SBV Journal of Basic, Clinical and Applied Health Science (2020): 10.5005/jp-journals-10082-02234.
- [39]Bergenstal RM, Johnson M, Powers MA, Wynne A, Vlajnic A, et al. Adjust to target in type 2 diabetes: comparison of a simple algorithm with carbohydrate counting for adjustment of mealtime insulin glulisine. Diabetes Care. 2008 Jul;31(7):1305-10. doi: 10.2337/dc07-2137. Epub 2008 Mar 25.
- [40]Lee Y, Siddiqui WJ. Cholesterol Levels. [Updated 2021 Jul 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan.
- [41]Durrington P. Dyslipidaemia. Lancet. 2003 Aug 30;362(9385):717-31. doi:10.1016/S0140-6736(03)14234-1.
- [42]Agarwal AK, Singla S, Singla S, Singla R, Lal A, Wardhan H, et al. Prevalence of coronary risk factors in type 2 diabetics without manifestations of overt coronary heart disease. J Assoc Physicians India. 2009, 57:135-42.
- [43]Bhardwaj S, Misra A, Misra R, Goel K, Bhatt SP, Rastogi K, et al. High prevalence of abdominal, intra-abdominal and subcutaneous adiposity and clustering of risk factors among urban Asian Indians in North India. PLoS One. 2011;6(9): e24362. doi: 10.1371/journal.pone.0024362.
- [44]Shahwan MJ, Jairoun AA, Farajallah A, Shanabli S. Prevalence of dyslipidemia and factors affecting lipid profie in patients with type 2 diabetes. Diabetes Metab Syndr. 2019 Jul-Aug;13(4):2387-2392. doi: 10.1016/j.dsx.2019.06.009.
- [45]Brijesh M. Diabetes mellitus and dyslipidemia: A detailed analysis. International Journal of Diabetes Sciences, 2019, Volume 1; Issue 1; January.
- [46]Surendra NB, Shubhransu P. Dyslipidaemia pattern amongst diabetic patients visiting a tertiary care hospital in Eastern Odisha. Int J Adv Med. 2017, 4(6):1662-1667. doi: 10.18203/2349-3933.ijam20175186.
- [47]Hu D, Jablonski KA, Sparling YH, Robbins DC, Lee ET, Welty TK, Howard BV. Accuracy of lipoprotein lipids and apoproteins in predicting coronary heart disease in diabetic American Indians. The Strong Heart Study. Ann Epidemiol. 2002 Feb;12(2):79-85. doi: 10.1016/s1047-2797(01)00208-3.
- [48]Manley SE, Stratton IM, Cull CA, Frighi V, Eeley EA, Matthews DR, et al. Effects of three months’ diet after diagnosis of Type 2 diabetes on plasma lipids and lipoproteins (UKPDS 45). UK Prospective Diabetes Study Group. Diabet Med. 2000 Jul;17(7):518-23. doi: 10.1046/j.1464-5491.2000.00320. x.
- [49]Li CM, Bai WJ, Liu YT, Tang H, Rao L. Dissipative energy loss within the left ventricle detected by vector flow mapping in diabetic patients with controlled and uncontrolled blood glucose levels. Int J Cardiovasc Imaging. 2017 Aug;33(8):1151-1158. doi: 10.1007/s10554-017-1100-8.
- [50]Amos AF, McCarty DJ, Zimmet P. The rising global burden of diabetes and its complications: estimates and projections to the year 2010. Diabet Med. 1997;14 Suppl 5: S1-85.
- [51]Kameran HI, “Lipid profile of controlled and uncontrolled diabetics in Erbil, Iraq”, Iraqi journal of community medicine. 2016, Volume 29, Issue 4.
- [52]Murwan KS, Mohammed AA, Atif Saeed MI, Ali Abdel-Ghaffar ARM, Mohammed Abdel RI. A Study of Lipid Profile Levels of Type II Diabetes Mellitus, Nova Journal of Medical and Biological Sciences, 2016, Vol. 5(2). doi: 10.20286/nova-jmbs-050203.
- [53]Del PS, Bonadonna RC, Bonora E, Gulli G, Solini A, Shank M, et al. Characterization of cellular defects of insulin action in type 2 (non-insulin-dependent) diabetes mellitus. J Clin Invest. 2013 Feb;91(2):484-94.
- [54]Li FR, Yang HL, Zhou R, Zheng JZ, Chen GC, Zou MC, et all. Diabetes duration and glycaemic control as predictors of cardiovascular disease and mortality. Diabetes Obes Metab. 2021 Jun;23(6):1361-1370.
- [55]Otamere HO, Aloamaka CP, Okokhere PO, Adisa WA. Lipid profile in diabetes mellitus; What impact has age and duration. British Journal of Pharmacology and Toxicology, 2011, 2(3): 135-137.