Effect of KISS1 gene variants (rs372790354 G>A and rs4889 G>A) on kisspeptin in patients with polycystic ovary syndrome in Iraq
Abstract
Polycystic ovary syndrome (PCOS) is a heterogeneous genetic disorder categorized by hyperandrogenism that affects early reproductive age in females. KISS1 has played role in regulating the hypothalamic-pituitary-gonad axis. It also plays a key role in human reproductive function. Imbalance-of-function mutations is often found KISS1 gene of patients with polycystic ovary syndrome. Blood samples were collected from 120 patients (60 control are divided into 30 normal weight and 30 obese) and (60 PCOS) females are divided into 30 normal weight and 30 obese. DNA was extracted and genotyped for KISS1 variants by HRM-PCR and measured the level of kisspeptin by ELIAS, while LH, FSH, DHEA and free testosterone by CLIA. The value of LH, Testosterone, DHEA-S and kisspeptin is elevated in the patient group, while the decline of FSH in serum level patients value, rs372790354 G > A and rs4889 G>A was associated with PCOS in dominant, recessive, co-dominant (P-value< 0.05), rs37279054 AA was not found the effect of obese group and linked with normal weight PCOS put present study no effect on the parameters, rs4889 GG/GA was the effect on all subgroups except the genotype GA not effected on obese female, the highly significant ( P-value<0.05) of rs4889 GA influenced on measured of WHR, LH/FSH ratio and DHEA-S in the patient compared to control, rs4889 GG/AA was influenced on normal-weight patient compare to an obese patient, the WHR was higher in an obese patient in both genotype. While the level of kisspeptin in normal weight with genotype AA was higher level compared to obese and (P-value<0.05). We concluded that the KISS1 levels were higher in PCOS females compared to controls and decreased with increasing BMI, KISS1 polymorphism rs372790354 G>A and rs4889 G>A may be associated with the pathophysiology of PCOS and lead to increased serum level of LH that due to hyperandrogenism.
INTRODUCTION
Polycystic ovary syndrome (PCOS) is one of the most common endocrine disorders characterized by multiple hormonal imbalances. Increased gonadotrophin-releasing hormone (GnRH) pulsatility in the hypothalamus increases luteinizing hormone (LH) secretion from the pituitary gland, leading to ovarian hyperandrogenism, ovulatory dysfunction(irregular menstrual cycle), and polycystic ovarian (PCO) morphology that affects at early reproductive age [1]. The National Institutes of Health (NIH) in 1990, the Rotterdam criteria (ROT) in 2003, and the Androgen Excess and PCOS Association (AE-PCOS) in 2006 used and developed three distinct ways to diagnose the condition [2]. The prevalence of PCOS is estimated at 4% to 8% [3] [4]. The diagnostic criteria for PCOS, according to the AE-PCOS Society, included polycystic ovaries (≥12 small follicles in the ovary) and/or ovarian dysfunction: ovulatory dysfunction (oligo or amenorrhea, infertility), less than 6-9 menstruation per year [3,5], and clinical and/or biochemical hyperandrogenism such as hirsutism, acne and androgenic alopecia (modified Ferriman-Gallwey score >8) [6].
The KISS1 gene is one of the candidate genes contributing to a regulatory role in the female reproductive system. KISS1 plays a vital role in gonadotropin secretion of the HPG axis [5]. It is located on the long arm of chromosome1 (1q32.1), length: 6,151 nucleotides, gene ID: 3814. The human KISS1 mRNA is transcribed from the KISS1 gene. The transcription involves four exons, of which only the third and fourth exons are to end translated into the sequencing of 145 amino acids as a peptide called kisspeptin-145. Subsequently, it is cleaved into four formulas of active kisspeptin consisting of 13, 14, 54, and 10 amino acids [5,7]. Some single nucleotide polymorphisms (SNPs) found in the KISS1 gene affect healthy female reproductive system function by interfering with the HPG axis, which plays an essential key in PCOS etiopathogenesis such as the missense effect [6].
Because disorders that simulate PCOS are relatively easy to rule out, all females have their TSH and prolactin levels checked. Amenorrhea or oligomenorrhea are two symptoms of hyperprolactinemia [7]. Menstrual irregularities are a symptom of thyroid illness. Non-classical congenital adrenal hyperplasia should be checked out in females with hyperandrogenism, as it occurs in 1.5% to 6.8% of these individuals. Other disorders, such as Cushing’s syndrome, should be investigated, and the 17-OHP level should be evaluated in the selected female with amenorrhea [8,9]. PCOS is caused by a dysfunctional interaction of behavior, environmental, and hereditary variables. The most typical clinical presentation of PCOS includes enlargement of both ovaries and secretion of androgens levels higher than normal theca cells. Enzymatic hyperactivity involved in steroid synthesis causes increased androgenic secretion. Defects of the hypothalamic-pituitary-ovarian axis, including intra-ovarian, autocrine/paracrine managers [10]. Instead, regulators outside the reproductive axis may be involved in the genesis and conservation of hypersecretion of LH, the thecal-stromal cell hyperactivity, and hypofunction of the FSH-granulosa cell axis. Resulting in hyperandrogenism and ovarian dysfunction [11]. Hypothalamic kisspeptin neurons (products of the KISS1 gene) acting via G protein-coupled receptor 54 (GPR54) are localized in two regions: the anterior and the posterior region of the hypothalamus [12]. Kisspeptin secretion further regulates the pulsatile release of GnRH and LH [13]. In the pathogenesis of the polycystic ovarian disease, abnormality in the hypothalamic-pituitary-ovarian or adrenal axis has been imposed. The relative increase in LH to FSH release is caused by a disruption in the secretion pattern of the gonadotropin-releasing hormone (GnRH) [14-18].
MATERIALS AND METHODS
Sample collection
blood samples were collected from 120 patients (60 control are divided into 30 normal weight and 30 obese) and (60 PCOS females are divided into 30 normal weight and 30 obese). The blood was collected from the females with PCOS between the second and fifth day of the cycle, and the patients were selected according to AE PCOS criteria. Using the Ferriman–Gallwey scale, a physical examination and hirsutism assessment were performed on all patients after obtaining their medical histories. Ferriman–Gallwey scale is a method of evaluating and quantifying hirsutism in women. The method was originally published in 1961 by D. Ferriman and J.D. Gallwey in the Journal of Clinical Endocrinology. The original method used 11 body areas to assess hair growth but was decreased to 9 body areas [19] .female having other causes of hyperandrogenism or menstrual irregular were excluded as hyper prolactinoma, Cushing disease, congenital adrenal hyperplasia, and female was pregnancy.
Ethical statement
Every volunteer has given written informed permission. This research received ethical approval (DSM/HO-65031) for scientific research from the Ministry of Health MOH and Ministry of Higher Education and Scientific Research MOHESR ethics committees in Iraq.
Biochemical analysis
Follicle Stimulating Hormone (FSH) and Luteinizing Hormone (LH) were measured by Chemiluminescence (CLIA), kisspeptin was determined by enzyme-linked immunosorbent assay (ELISA) kit, were performed in the University of Babylon medicine collage. In the extraction of DNA from fresh whole blood, the concentration and purity of the DNA were determined by using a nanodrop spectrophotometer by G-spin kit, SNPs of KISS1 gene determination and using real-time PCR to amplify the KISS1 gene. Then by HRM technique to a genotyping analysis using the following amplification primer and positive and negative control.
Table 1 showed the PCR primer for genotyping of KISS1 gene rs372790354 alleles: G>A and rs4889 alleles G>A, and Table 2 showed the PCR Condition for genotyping of KISS1 gene rs372790354 alleles: G>A and rs4889 alleles G>A.
Table 1. PCR primer for genotyping of KISS1 gene rs372790354 alleles: G>A and rs4889 alleles G>A.
Table 2. PCR Condition for genotyping of KISS1 gene rs372790354 alleles: G>A and rs4889 alleles G>A.
Statistical analysis
Statistical calculations were performed using the statistical software SPSS version 23. Data descriptive are communicated as the mean ± standard error (Mean± SE); the ANOVA test was used to compare the mean value between subgroups to investigate the correlation between the continuous variables using Pearson’s correlation statistics. The hormonal level was compared between control and patient with PCOS (normal and obese). considered P-value of < 0.05 statistically significant.
Genotype and allele frequency of KISS1 gene polymorphism were calculated, and consequently, the Hardy-Weinberg equilibrium, Chi square (x2) test was used for categorical variables.
RESULTS
Biochemical assay
Table 3 showed the demographic distribution of the study groups. No significant changes in age and BMI were seen between PCOS patients and the control groups. In this investigation, WHR was significantly different across the studied groups.
Table 4 showed the mean difference and comparison of hormonal parameters between the subgroups, where the biochemical markers are also different between the patients and the control group. In PCOS, LH and DHEAS are high, whereas FSH is decreased compared to control groups (normal weight and obese), and kisspeptin was significantly higher in normal-weight PCOS compared to other subgroups.
Table 5 showed the correlation coefficients between the level of parameters in normal weight and obese patients. There are significant correlations between hormonal parameters in normal-weight PCOS, which showed positive correlations between LH with LH/FSH Ratio, LH with kisspeptin, and LH/FSH Ratio with kisspeptin, while found a negative correlation between FSH with LH/FSH ratio.
Table 3. Demographic data of studied groups.
Table 4. Mean difference and comparison of hormonal parameters between the subgroups.
Table 5. Correlation coefficients between level of parameters in normal and obese patients.
Genotyping assay
Table 6 showed the gene polymorphism of KISS1 in studied groups for rs372790354 G>A. When comparing the (genotype and allele frequency) for each SNP between PCOS females and controls, Hardy-Weinberg equilibrium was applied to the control groups (P>0.05). A novel SNPs homozygous (GG), heterozygosis (GA), and mutant (AA) of both SNPs information. Figure 1 showed the amplification and genotype of rs372790354 G>A for Control and Samples. Figure 2 showed the amplification and genotype of rs4889 G>A for Control and Samples. Table 7 showed the association of rs372790354 genotypes with PCOS under different inheritance models. Significant differences were exhibited in the co-dominant model for GG, GA, and AA groups at (0.026 and 0.0036), respectively. In the dominant model, significant differences showed for GG and GA-AA groups at (0.0021), respectively. In the recessive model, significant differences showed for GG- GA and AA groups at (0.011), respectively. In contrast, there are no significant differences in over dominant model for AA-GG and GA groups.
Table 8 showed the distribution of genotype frequency of rs372790354 G>A of KISS1 gene polymorphism between patient and control group within subgroup normal weight and obese where there are significant differences for AA group at 0.059.
Table 9 showed the association of rs4889 genotypes with PCOS under different models of inheritance where there are significant differences in the co-dominant model for GG, GA, and AA groups at (0.0003 and 0.0004), respectively. In the dominant model, significant differences showed for GG and GA-AA groups at (0.0001), respectively. In the recessive model, significant differences showed for GG- GA and AA groups at (0.0035), respectively. Finally, the Over dominant model for AA-GG and GA groups showed significant differences at (0.04).
Table 10 showed the distribution of genotype frequency of rs4889 G>A of KISS1 gene polymorphism between patient and control group within normal subgroup weight and obese. Significant differences in GA type for normal weight at (0.0002 and 0.0042), respectively, while there are no significant differences in the obese group. In AA type, there are significant differences between the normal-weight group at (0.0007 and 0.07) and the obese group at (0.03), respectively.
Table 11 showed the alleles frequency and allelic association of rs372790354 G>A and rs4889G>A by Hardy-Weinberg equilibrium law of KISS1 gene polymorphism between the patient group and control group. Where there are significant differences in rs372790354 SNP for G allele at (0.0002) and odd ratio value (0.34) between 0.2 – 0.5, While for A allele at (0.0002) and odd ratio value (2.96) between 1.68 – 5.19. In rs4889 SNP, there are significant differences for the G allele at (< 0.0001) and odd ratio value (0.2) between 0.1 – 0.3. While for the A allele at (< 0.0001) and odd ratio value (4.9) between 2.7 – 8.8.
Table 12 showed the influence of rs4889 G>A polymorphism of KISS1 gene on the Mean differences of characteristics and parameters between genotypes normal weight (patient and control) groups. Where there are significant differences for WHR, LH/FSH Ratio, F-Testosterone, and DHEA-S markers at (<0.01) for all of them, while there are no significant differences for LH, FSH, and kisspeptin markers
Table 13 showed the influence of rs4889 G>A polymorphism of KISS1 gene on the Mean differences of characteristics and parameters between genotypes patient (normal weight and obese) groups. There are significant differences for WHR, and kisspeptin markers at (<0.01 and 0.007), respectively, while there are no significant differences for LH, FSH, Ratio FSH/LH F-Testosterone, and DHEA-S markers.
Table 14 showed the Genotype combination of SNPs rs4889 and rs372790354 in the KISS1 gene between the patient group and control group (Allele Frequencies detected by Hardy-Weinberg equilibrium law). There are no significant differences for rs4889 + rs372790354 SNPs for all groups under study depending on P-value and odd ratio Hardy-Weinberg equilibrium.
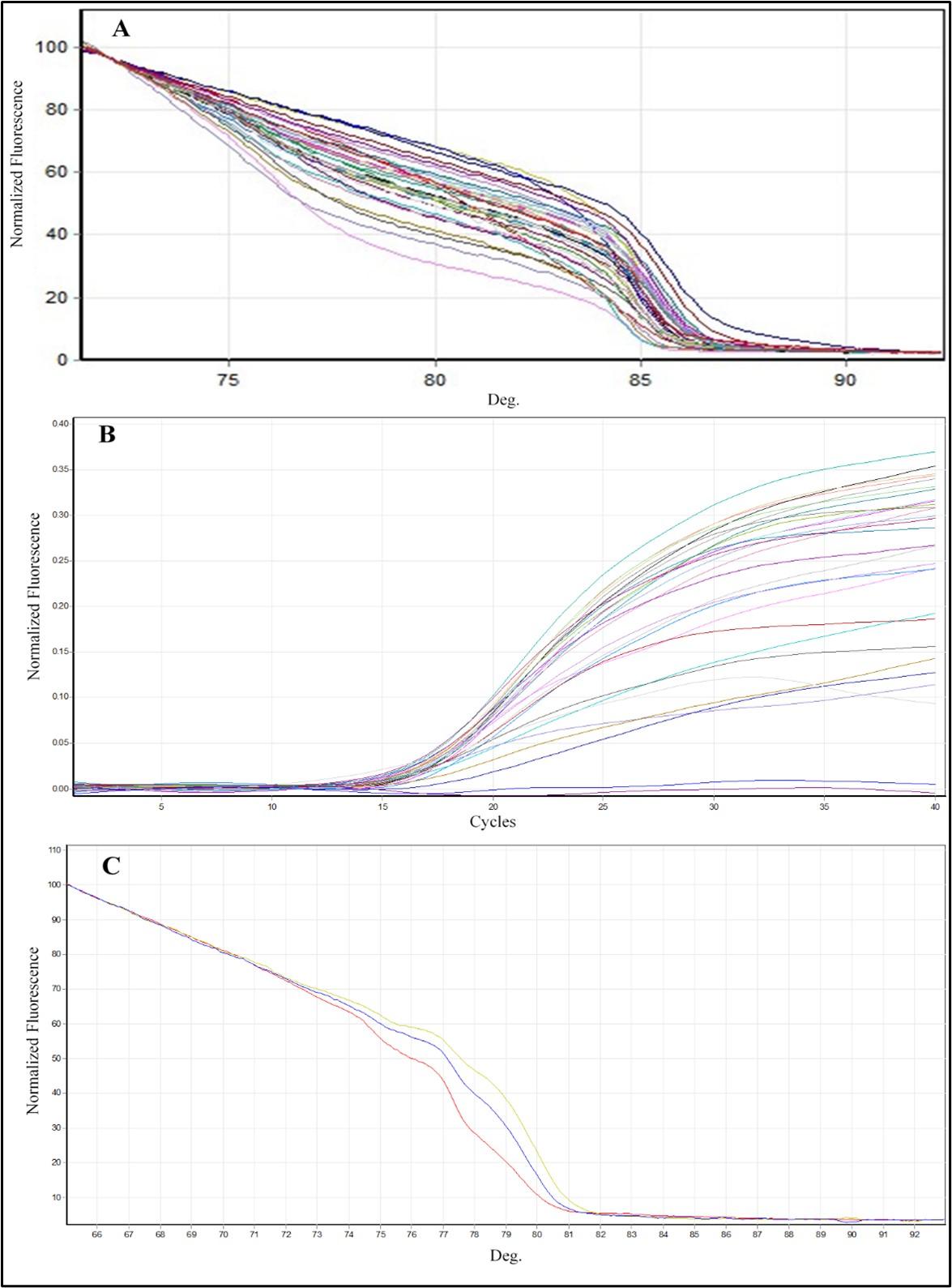
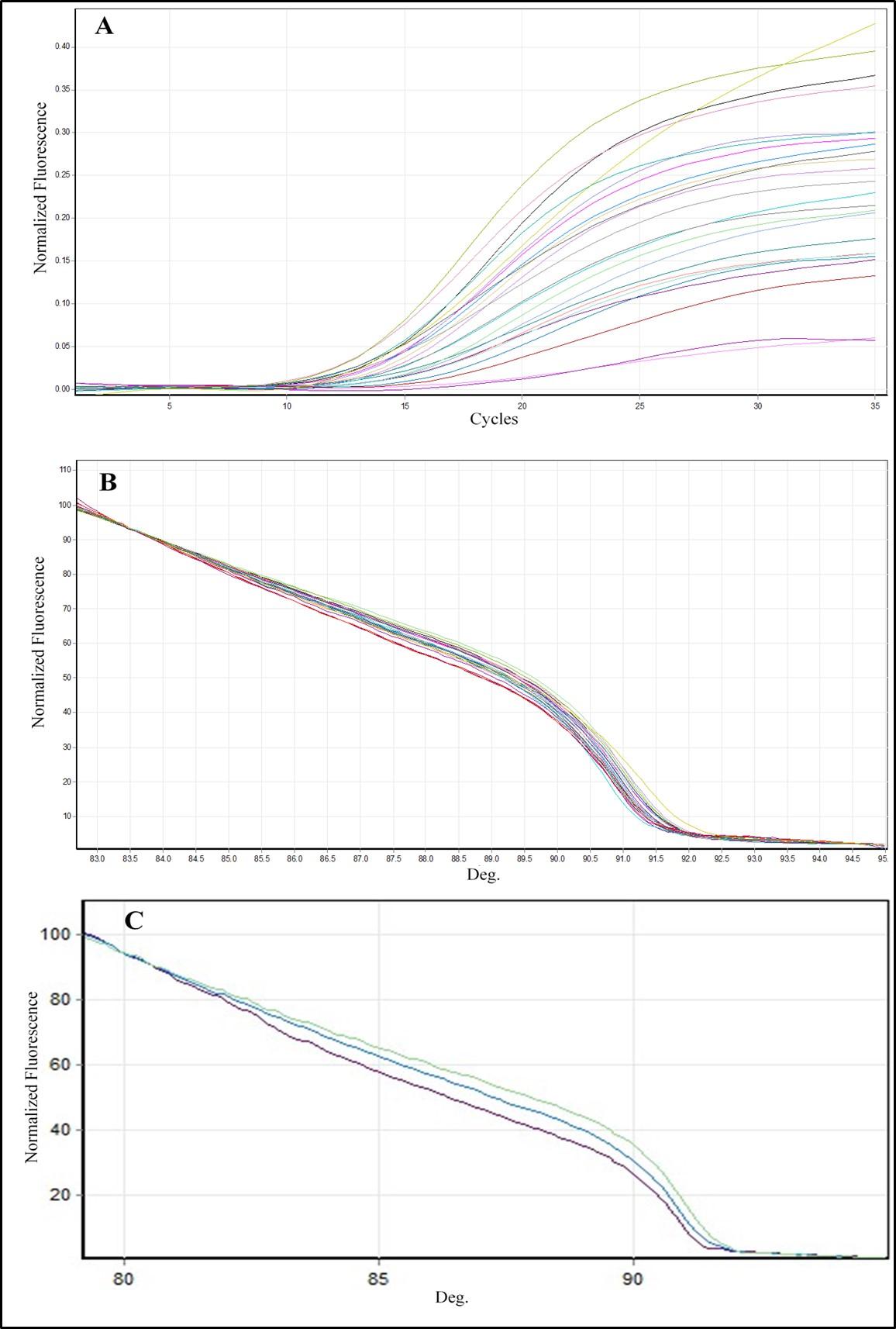
Table 6. Gene polymorphism of KISS1 in studied groups.
Table 7. Association of rs372790354 genotypes with PCOS under different models of inheritance.
Table 8. Distribution to genotype frequency of rs372790354 G>A of KISS1 gene polymorphism between patient and control group within normal subgroup weight and obese.
Table 9. Association of rs4889 genotypes with PCOS under different models of inheritance.
Table 10. Distribution to genotype frequency of rs4889 G>A of KISS1 gene polymorphism between patient and control group within normal subgroup weight and obese.
Table 11. Allele’s frequency and allelic association of rs372790354 G>A and rs4889G>A by Hardy-Weinberg equilibrium law of KISS1 gene polymorphism between patient group and control group.
Table 12. The influence of rs4889 G>A polymorphism of KISS1 gene on the mean difference of characteristics and parameters between genotypes normal weight (patient and control) group.
Table 13. The influence of rs4889 G>A polymorphism of KISS1 gene on the mean differences of characteristics and parameters between genotypes patient (normal weight and obese) group.
Table14. Genotype combination of SNPs rs4889 and rs372790354 in KISS1 gene between patient group and control group (Allele Frequencies detected by Hardy-Weinberg equilibrium law).
DISCUSSION
The disturbance in Hypothalamus-Pituitary-Gonadal (HPG) axis is related to PCOS. Kisspeptin is a neuropeptide expressed by the KISS1 gene that has a highly active action on the HPG axis and plays a crucial role in human reproduction [20]. KISS1 gene is mainly expressed in the hypothalamus to the secretion of GnRH that is regulatory of LH and FSH, the genetic factor responsible for the etiopathogenesis of PCOS [21]. The present study investigated KISS1 gene polymorphism which could be used as a marker of PCOS and its risk factor in Iraqi females. Two novel SNPs (rs372790354G>A and rs4889 G>A) in the KISS1 gene were identified and investigated in this study. The effect of the two SNPs was studied by analyzing and comparing genotype groups, which leads to endocrine disturbances (kisspeptin, LH, FSH, LH/FSH ratio, and DHEA-S) in the female with PCOS.
The result of demographic data was shown in Table 1 that there was no significant difference in mean age and BMI between the studied group. At the same time, there was a highly significant difference in mean WHR. The present study showed in Table 2 that the level of kisspeptin was slightly higher in females obese without PCOS compared to the obese female with PCOS group were not significantly different, supporting these findings by Yerlikaya et al. [22]. The mean of kisspeptin in obese females with and without PCOS was approximately the same. It may be due to the stimulatory action of obesity on kisspeptin neurons, which are also regulated by leptin, insulin resistance, ghrelin, and adiponectin (excitatory) (inhibitory) [20]. The current study showed a higher significance in the mean of normal-weight patients compared to control and obese patient (P-value <0.01). Three previous studies[23–25] reported a higher kisspeptin level in females with PCOS. Another study [26] reported lower levels in females with PCOS compared to controls. Nearmeen and her colleagues found that kisspeptin levels among the PCOS group there was a significantly lower level in the underweight, overweight, and obese compared to the normal weight group [27].
In the present study, table 2 showed that LH values were higher in PCOS females than in controls. High levels of LH contribute to increasing levels of androgens along with low levels of FSH secretion compared to the control group [28]. These data suggest that endocrine hormone concentrations were significantly higher in PCOS [29]. The present study shows PCOS females with high BMI have elevated androgen levels.
The correlation between biochemical parameters of PCOS patients, as shown in Table 3, serum kisspeptin was positively correlated with the LH and LH/FSH ratio in normal-weight patients and with LH/FSH ratio only in the obese patients. Also, DHEA positively correlated with LH and FSH levels in obese patients. Obesity, insulin resistance, and dyslipidemia are PCOS-related morbidities that correlate with the LH/FSH ratio. Kisspeptin may stimulate LH secretion. In the normal patients, kisspeptin is higher than in the obese group, leading to higher LH levels in normal-weight than in obese. However, the directed pituitary effects of kisspeptin in regulating gonadotropin secretion remain controversial [30]. In all models, the genotype (homozygous AA and heterozygous GA) of rs372790354 and rs4889 (homozygous AA and heterozygous GA) was significantly (P 0.05) more frequent in PCOS than in controls (Table 5 and 7). While within subgroups, rs372790354 (AA) is highly significant (P-value<0.001) in normal-weight patients as a compared to normal-weight control. That means the SNP link to PCOS as shown in Table 6, rs372790354 genotype AA normal weight patients showed no significant influence on the value of demographic characteristics and endocrine (the result are not shown). The SNP rs372791354 does not influence the level of kisspeptin and other hormones. There was no difference in its level in the two different genotypes of rs372790354.
These findings disagree with the results of Maha and his colleagues [31], which showed a significant influence of rs372790354 G/A on the risk of PCOS and the increase of LH levels, kisspeptin, and WHR in PCOS females. Maybe this SNP is located in 5 prime untranslated regions of the mRNA KISS1 gene that have both stimulatory and inhibitory mechanisms, including regulation of mRNA transcription and post-transcriptional modification (secondary structure and mRNA stability), localization, and mRNA translation. It also regulates protein features such as protein complex formation and post-translational modifications and may alter protein conformation [23, 24]. That means affecting kisspeptin conformation or its binding to the receptor. Therefore, this SNP with two genotypes has higher significant frequencies and risk factors associated with PCOS.
Allele frequency of rs372790354 G>A and rs4889G>A were also significant in both SNPs. The mutant had a higher predisposition (P<0.05) in patient groups compared with control, and the allele G was protective, as shown in Table 9. The rs4889 GA and AA have a higher frequency in normal-weight patients compared to the obese patients, and all subgroups of control as shown in Table 8, except the genotype GA was not significant in obese with PCOS compared to obese without PCOS. Polymorphism of rs4889 introduced a substitution of proline at the 81 positions. This substitution was observed in kisspeptin-54 but not in the other three forms of kisspeptin (kisspeptin-14, -13,-10) [34].
The result of rs4889 genotype AA and GA between patient and control, normal weight, and the obese patient is shown in Tables 10 and 11. The obesity-linked parameters that have influenced the pathology of PCOS, including WHR, were significantly in PCOS groups with genotype GA compared to control and significantly higher in ( obese compared to normal weight ) patients with genotype GA, AA. In other studies, the allele C instead of allele A for this SNP. These findings confirm the results of Mazin and his colleagues’ study [35]. The importance of WHR as a prognostic marker, higher WHR in PCOS compared to obese control, confirms the contribution of abdominal fat as an etiological mechanism in PCOS. The PCOS genotype GA group showed the feature of endocrine disturbances that increase the value of LH/FSH ratio and DHEA-S (P-value =0.01).
In contrast, kisspeptin, FSH, and LH showed no significant difference compared to GA genotype control. In addition, higher levels of kisspeptin (normal weight compared to obese P-value= 0.007) were found in patients with genotype AA. In a previous study, Albalawi and his colleagues reported no significant difference in the kisspeptin level between PCOS females and controls [34].
No significant elevation of the kisspeptin level in PCOS patients may be due to the low sample size. The effect of rs4889 GA and AA polymorphism of the KISS1 gene may directly impact the functional activity of kisspeptin in terms of its altered behavior and binding capacity of kisspeptin to its receptor GPR54 [35]. Consequently, the disturbed kisspeptin-GPR54 pathway and dysregulation in GnRH secretion lead to LH hypersecretion, leading to hyperandrogenism. Increased testosterone level is induced by the direct action of high stimulation of LH on gonads; it appears that rs4889 influences the mechanism by which kisspeptin activates the secretion of LH but not FSH [36]. Finally, the females with both AA and GA genotypes from the two SNPs in this study have a higher risk of developing PCOS.
CONCLUSION
We concluded that the KISS1 levels were higher in PCOS females compared to controls and lowered with increasing BMI. Consequently, the value of kisspeptin is higher in normal-weight patients compared to obese females. KISS1 polymorphism rs372790354 G>A and rs4889 G>A may be associated with the pathophysiology of PCOS and lead to the increased serum level of LH due to hyperandrogenism; rs4889 AA may cause hyperactivity of the KISS1 gene.
ACKNOWLEDGEMENT
The authors would like to thank Dr. Yasir Haider Al-Mawlah and Dr. Ameer Mezher Hadi (DNA Research Center, University of Babylon. Pune for their kind support with all laboratory equipment and provide the suitable facilities, also for drafting the manuscript to make this work done.
AUTHOR CONTRIBUTIONS
Conception and design of the study: Noor J. T. Al-Musawi, Suhayr Aesa Al- Qaysi, and Suha J. Witwit; Drafting the manuscript: Suhayr Aesa Al- Qaysi; Analysis and/or interpretation of data: Suha J. Witwit.
CONFLICTS OF INTEREST
There is no conflict of interest among the authors.
References
- [1]Branavan U, Muneeswaran K, Wijesundera S. Identification of selected genetic polymorphisms in polycystic ovary syndrome in Sri Lankan women using low-cost genotyping techniques. PLoS One 2018; 13(12): e0209830.
- [2]H. Chaudhary, J. Patel, N. K. Jain, et al. The role of polymorphism in various potential genes on polycystic ovary syndrome susceptibility and pathogenesis. Journal of Ovarian Research 2021; vol. 14, no. 1.
- [3]F. A. K. Khazaal, A. H. Liebi, and I. J. Mahmoud. Prevalence and presenting features of polycystic ovarian syndrome in Iraqi obese females. Iraqi journal of infertility research, baghdad 2014; pp. 14–18.
- [4]W. A. March, V. M. Moore, K. J. Willson, et al. The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria Wendy. original article reproductive epidemiology 2011; pp. 544–551.
- [5]Kiconco, Sylvia, Mousa et al. Pcos phenotype in unselected populations study (P-pup): Protocol for a systematic review and defining pcos diagnostic features with pooled individual participant data. Diagnostics 2021; vol. 11, no. 11.
- [6]M. K. C. C. Ilagan, E. Paz-Pacheco, D. Z. Totesora, et al. The modified Ferriman-Gallwey score and hirsutism among Filipino women. Endocrinology and Metabolism 2019; vol. 34, no. 4. pp. 374–381, 2019
- [7]Vermeulen And S. Ando. Prolactin and adrenal androgen secretion. Clinical Endocrinology 1978; vol. 8, no. 4. pp. 295–303.
- [8]E. Jones. Diagnosis and treatment of polycystic ovarian syndrome. Nursing times 2005; vol. 101, no. 3. pp. 40–43.
- [9]Paul W. Ladenson, MD, Peter A. Singer, MD, Kenneth B. Ain, MD, et al. American thyroid association guidelines for detection of thyroid dysfunction. Archives of Internal Medicine 2000; vol. 160, no. 11. pp. 1573–1575. 10.1001/archinte.160.11.1573.DOI: 10.1001/archinte.160.11.1573.
- [10]Gerard Conway, Didier Dewailly, Evanthia Diamanti-Kandarakis, et al. The polycystic ovary syndrome: a position statement from the European Society of Endocrinology Gerard. 2015; no. 8 (72).
- [11]J. Morales, G. A. Laughlin, T. Bijtzow, H. Maheshwari, et al. Insulin, somatotropic, and luteinizing hormone in lean and obese women with polycystic ovary syndrome: Common and distinct features Axes A. 1996;
- [12]J. Roa, J. M. Castellano, V. M. Navarro, et al. Kisspeptins and the control of gonadotropin secretion in male and female rodents. Peptides, 2009; vol. 30, no. 1. pp. 57–66. 10.1016/j.peptides.2008.08.009.
- [13]N. Bhalakiya, N. Haque, and P. Patel. Kisspeptin: A novel regulator in reproductive physiology. Int. J. Livest. Res.2019; p. 1.
- [14]Z. Saadia. Follicle stimulating hormone (LH: FSH) ratio in polycystic ovary syndrome (PCOS) – obese vs. non- obese women. Medical archives (Sarajevo, Bosnia and Herzegovina)2020; vol. 74, no. 4. pp. 289–293.
- [15]S. Z. Nejad, F. R. Tehrani, and A. Zadeh-Vakili. The role of kisspeptin in female reproduction. International Journal of Endocrinology and Metabolism 2017; vol. 15, no. 3.
- [16]E. Oakley, D. K. Clifton, and R. A. Steiner. Kisspeptin signaling in the brain. Endocrine Reviews2009; vol. 30, no. 6. pp. 713–743.
- [17]NCBI, “KISS1 gene location.” [Online]. Available: https://www.ncbi.nlm.nih.gov/gene/3814. [Accessed: 29-Mar-2022].
- [18]“Kisspeptin structure.” [Online]. Available: https://www.uniprot.org/uniprot/Q15726#showFeaturesTable. [Accessed: 29-Mar-2022].
- [19]G. J. Ferriman David. Clinical assessment of body hair in women. J Clin Endocrinol Meta., 1961; vol. 21, no. January. pp. 1440–7.
- [20]J. Padda et al. Role of kisspeptin on hypothalamic-pituitary-gonadal pathology and its effect on reproduction. Cureus. 2021.
- [21]O. Valkenburg et al. Genetic polymorphisms of GnRH and gonadotrophic hormone receptors affect the phenotype of polycystic ovary syndrome. Hum. Reprod.2009; vol. 24, no. 8, pp. 2014–2022.
- [22]E. Yerlikaya et al. Plasma kisspeptin levels in polycystic ovary syndrome. in Endocrine Abstracts 2013; vol. 32.
- [23]S. A. Yilmaz. Metastin levels in relation with hormonal and metabolic profile in patients with polycystic ovary syndrom. Eur. J. Obstet. Gynecol. Reprod. Biol.2014; vol. 180, no. 1, pp. 56–60.
- [24]X. Chen, Y. Mo, L. Li, et al. Increased plasma metastin levels in adolescent women with polycystic ovary syndrome. Eur. J. Obstet. Gynecol. Reprod. Biol.2010; vol. 149, no. 1, pp. 72–76.
- [25]Y. E. Jeon et al. Kisspeptin, leptin, and retinol-binding protein 4 in women with polycystic ovary syndrome. Gynecol. Obstet. Invest.,2013; vol. 75, no. 4, pp. 268–274.
- [26]D. Panidis et al. Plasma metastin levels are negatively correlated with insulin resistance and free androgens in women with polycystic ovary syndrome. Fertil. Steril.2006; vol. 85, no. 6, pp. 1778–1783.
- [27]N. M. Rashad, R. M. Al-sayed, M. S. Yousef, et al. Kisspeptin and body weight homeostasis in relation to phenotypic features of polycystic ovary syndrome; metabolic regulation of reproduction. Diabetes Metab. Syndr. Clin. Res. Rev.2019; vol. 13, no. 3, pp. 2086–2092.
- [28]Z. Guleken, H. Bulut, P. Y. Bahat, et al. Elevated serum level of DHEAS as a hormone and IL-6 as a proinflammatory cytokine may better indicate metabolic syndrome in PCOS women. J. Med. Physiol. Biophys. 2021.
- [29]Yuan, X. Liu, Y. Mao, F. et al. Polycystic ovary syndrome patients with high BMI tend to have functional disorders of androgen excess: A prospective study. Journal of Biomedical Research 2016; vol. 30, no. 3. pp. 197–202.
- [30]J. M. Castellano. Changes in hypothalamic KiSS-1 system and restoration of pubertal activation of the reproductive axis by kisspeptin in undernutrition. Endocrinology 2005; vol. 146, no. 9, pp. 3917–3925.
- [31]M. H. Daghestani. Influence of KISS1 gene polymorphisms on the risk of polycystic ovary syndrome and its associated variables, in Saudi women. British Journal of Biomedical Science2020; vol. 77, no. 4. pp. 185–190.
- [32]Z. Lin and W. H. Li. Evolution of 5′ untranslated region length and gene expression reprogramming in yeasts. Mol. Biol. Evol.2012; vol. 29, no. 1, pp. 81–89.
- [33]Q. Fan et al. Functional polymorphism in the 5′-UTR of CR2 is associated with susceptibility to nasopharyngeal carcinoma. Oncology Reports 2013; vol. 30, no. 1. pp. 11–16.
- [34]F. S. Albalawi, M. H. Daghestani, M. H. Daghestani, et al. rs4889 polymorphism in KISS1 gene, its effect on polycystic ovary syndrome development and anthropometric and hormonal parameters in Saudi women. 2018.
- [35]M. H. Daghestani. Adverse effects of selected markers on the metabolic and endocrine profiles of obese women with and without PCOS. Front. Endocrinol. (Lausanne).2021; vol. 12.
- [36]K. Daghestani, M. H. Daghestani Mazin H. Daghistani, Mamoon. Ambreen. Relevance of KISS1 gene polymorphisms in susceptibility to polycystic ovary syndrome and its associated endocrine and metabolic disturbances. British Journal of Biomedical Science Journal 2020, 77(4):185-190